Dvora Pikkel1,2*
1Assuta Hospital, Ramat Hahayal, Tel-Aviv, Israel 2Ben Gurion University, Faculty of Medicine, Beer-Sheva, Israel
*Corresponding Author:Dvora Pikkel, Assuta Hospital, Ramat Hahayal, Tel-Aviv and Ben Gurion University, Faculty of Medicine, Beer-Sheva, Israel.
Received: February 25, 2021; Published: March 06, 2021;
Aim: To examine the microbial flora of the conjunctiva among hospital employees as a test case for assessing the degree that the hospital environment affects the microbiota of its inhabitants.
Methods: We took samples from the conjunctival sack (from both eyes) of hospital staff from different departments and incubated these samplesin order to find the existence of microbial flora. As a control group we tested in the same way people who were not exposed to hospital environment and had no conjunctivitis at the last 3 months. We compared the results of the 2 groups.
Results:The microbial flora of the conjunctiva did not differ between healthy health care professionals and a control group. However, greater bacteria incidence and diversity were found among staff in internal medicine wards compared to other departments.
Conclusion: In general, hospital staff are not in risk to be infected more than the regular population, however some of the people working at internal medical wards are more exposed to conjunctival contamination. A follow-up study of the participants of this work is needed to examine if re-current contamination is responsible for alterations in the conjunctival flora of health professionals; and a multi-center study is needed to confirm differences in bacteria incidence between hospital departments.
Keywords: Conjunctiva;Microbial Flora;Health Professionals;Hospital Environment;Recurrent Contamination;Bacterial Infection Incidence
Indoor environments and particularly those characterized by confinement and extensive cleanliness, such as hospitals, share certain microbiota features [1]. These include lower overall microbial diversity, greater diversity of resistance genes and an abundance of certain bacteria, including a shift from gram-positive to gram-negative [1,2]. The intensive use of various types of antibiotics in hospitals selects multi-resistant bacteria, which are usually not encountered in the general community [2]. Interactions of the microbiota of hospital facilities and of their inhabitants are two-way. Hospital staff, patients, and visitors represent the primary reservoir of normal microbiota in the hospital. Other sources include all environments in which nutrients, humidity, and temperature are suitable for bacteria survival, such as nebulizers, dialysis equipment, and food stored inadequately. Microbiota of indoor environments affect the microbiota of the people inhabiting them. Contact of an infectious agent with a host may be direct (hands or other organs), indirect (door knobs, robes, exam equipment) or by the projection of droplets (sneezing, coughing, or speaking). The risk of contacting a pathogenic infection in the hospital is higher and the chances of fatal consequences more serious than in other indoor environments [3]. This has promoted intensive study of bacteria in hospitals, such as in the Hospital Microbiome Project [4,5]. Hospital staff are particularly affected by the hospital microbiota. A yearlong investigation of bacteria on the hands of staff and patients in a newly constructed health facility showed that the microbiota of staff was more similar to that of surfaces in the hospital than were the patients’ microbiota [6].
The human eye is a sense organ that reacts to light and translates it to electrochemical signals [7,8]. Light entering the eye through the cornea and the pupil falls on the retina, where it initiates electric signals that are sent through fibers of the optical nerve to the visual cortex of the brain. Three structures protect the eye: the conjunctiva, the eyelids, and the lacrimal apparatus. The conjunctiva [7]is a thin and transparent mucous membrane that lines the inside surface of the lids. The epithelial layer contains blood vessels, fibrous tissue, and lymphatic channels. Accessory lacrimal glands in the conjunctiva help lubricate the eye by producing mucus and tears. Tears, which consist of such components as lysozyme, lactoferrin, beta-lysine, and IgG, constantly bathe the eyes. The combination of these components helps destroy bacteria. This explains the antibacterial action of tears, in addition to the mechanical removal of most organisms through the lacrimal ducts.
The microbial flora of the conjunctiva has been the subject of numerous studies [9-13]. The conjunctiva is first exposed to microbes when an infant passes through the birth canal, and immediately after, when the eye is exposed to environmental sources of bacteria such as air, contaminated material, and people. A hospital-based study in China reported a 24% incidence of conjunctiva bacteria [14]. The most abundant isolated bacteria are coagulase-negative Staphylococcus (Staphylococcus epidermidis), diphtheroids (Corynebacterium species), Propionibacterium acnesand Staphylococcus aureus[15-18];Streptococcus and gram-negative bacteria are also present. Among 45 healthy adults, examined twice at three-month intervals, no single taxa was found in all subjects, nor at both examinations [18]. The authors concluded that an overall core microbiome does not exist, though individuals tended to maintain some consistency in their microbiome.
Two mechanisms support the formation of microbe colonies in the eye [9]. Thefirst, colonization, is the establishment of an independent, stable, and constant community of microbes. Reproduction of the microbes is balanced by host-defenses,leading to a stable amount of microbes that persist for a long period without developing any infection. The second process, known as recurrent contamination, requires repeated introduction of microbes as host-defenses that reduce their levels and eventually eliminate their presence. Persistent or frequent contamination may result in an almost stable microbe population over a long period, similar to colonization. New microbes may be introduced from adjacent or distant tissues or from the environment. Therefore, under environmental changes, new microbes may temporarily or permanently become a part of the normal flora, without causing any damage. Due to its constant exposure to the environment, continuous contamination is the main source of microbes in the conjunctiva, and colonization is usually a minor component.
Constant exposure to the hospital environment may lead to changes in the normal flora of the conjunctiva of health professionals through the recurrent contamination mechanism as described above. A study conducted among 40 health professionals in Brazil [19] found changes in the flora of the conjunctiva compared to the normal flora as described in the literature. These findings confirm continuous contamination, while indicating that the mechanism of local defense continues to be intact, preventing the fixation of invading organisms. However, any change in the immunologic equilibrium may result in an infection. Bacterial conjunctivitis is generally self-limiting and does not require treatment [20]. Nonetheless, an infection may be difficult to treat due to the unique microbiota of the hospital environment, with its relative abundance of multi-resistant pathogens. Thus, understanding changes in the conjunctival microbiota is important for stress situations, for which specific prophylactic treatment might be needed to avoid infections and complications. Further, examination of the microbial flora of the conjunctiva of hospital employees can serve as a test case for assessing the degree that the hospital environment may endanger medical staff. In this study we compared between conjunctival flora of hospital employees and a control group, and between employees of different departments. We hypothesized that the flora would differ between the hospital employees and the control group, and between employees in different medical departments.
We sampled the conjunctival flora of hospital employees of different wards in a public hospital in northern Israel and compared it to the conjunctival flora of a group of students in an academic institute that has no connection with the hospital. The study was approved by the local bio-ethical committee of the hospital (Ziv 0093-12).
Research populationSamples were taken from clinically normal eyes of 50 health professionals (doctors and nurses), from five departments - internal medicine, surgery, intensive care, orthopedics, and geriatrics. All departments are from Ziv Medical Center, located in Safed, northern Israel. Ten professionals from each sector were selected randomly on a volunteer basis. Thirty adults who are not in daily contact with a hospital environment were selected on a volunteer basis and served as a control group. Inclusion criteria for participating in this research were: age above 18 years, not wearing contact lenses, no previous eye surgeries, and the absence of conjunctivitis in the subject and in close relatives in the past 3 months. For the control group, fewer than 4 visits to the hospital in the last 3 months was also an inclusion criterion.Each participant filled a questionnaire (see Appendix A) to verify meeting eligibility criteria.
This research was approved by the local Helsinki committee (0093-12-ZIV). Each participant signed a consent form to participate. The authors declare that they have no commercial or other adverse interest.
Sample analysisFour samples were taken from each participant - from the conjunctival sac and from the lacrimal punctum of each eye. The material was collected with sterile cotton swabs and kept at room temperature. A total of 200 samples were taken from the study group and 120 samples from the control group. The samples were then transferred for gram staining, to assess the presence of granulocyte cells or bacteria, and to distinguish between gram-negative and gram-positive bacteria. In addition, each sample was transferred to four types of growth medium: blood, chocolate, Mc-Conkey agar, and Thioglycolate broth. These plates were incubated at 37°Cin a CO2rich environment for 72 hours and analyzed on a daily basis using the Vitek 2 tool. A culture with no indication of growth was considered sterile.
Statistical methodsThe main variable of the research is the incidence of each bacteria in the studied population. Fisher’s Exact test was applied to compare bacteria incidence between the study and control groups, and between health professionals in different departments. A P-value of 5% or less was considered statistically significant. The data were analyzed using the SPSS version 20.0.0.2 (SPSS Inc. Chicago, IL, USA).
The data used to support the findings of this study may be released upon application to the corresponding author and is also attached as appendix to this article.
Bacteria were found in 27 of 100 eyes (27%) from 19 health professionals (38%) in the study group, and in 20 of 60 eyes(33%) from 11 participants (37%) in the control group (Table 1). No statistically significant differences were found in the presence of bacteria between these groups (P-value 0.087).
For both groups, coagulase-negative Staphylococcus was the predominant bacterium identified, presenting in 82% and 80% of the positive samples of the study and control groups, respectively (Table 1). Acinetobacter lwoffii, Staphylococcus aureus and Pseudomonas aeruginosa were found in very small numbers in both groups (Table 1).
| Study group (n=100) | Control group (n=60) | ||||
|---|---|---|---|---|---|
| Finding | N | % | N | % | P |
None |
73 |
73.0 |
40 |
66.7 |
0.087 |
Coagulase-negativeStaphylococcus |
22 |
22.0 |
16 |
26.7 |
|
Acinetobacter lwoffii+ Serratia liquefaciens |
2 |
2.0 |
2 |
3.3 |
|
Staphylococcus aureus |
2 |
2.0 |
1 |
1.7 |
|
Pseudomonas aeruginosa |
1 |
1.0 |
1 |
1.7 |
|
Table 1:The incidences of specific bacteria found in the study group (health professionals) and in the control group. N = number of eyes. Comparison using Fisher’s exact test yields P-value of 0.087.
Among the departments studied, internal medicine showed the largest number of contaminated eyes (Table 2), with 10 of 20 eyes (50%) positive for bacteria. The difference between this incidence and that of the other departments (surgery, geriatrics, and orthopedics) was statistically significant (P-value<0.05). Bacteria were found in only four eyes (20% of all eyes tested) in each of these three departments. Bacteria incidence was not significantly different between the ICU, where bacteria were found in 5 eyes (25%, P- value=0.071) and the control group, for whom bacteria were found in 20 eyes (33%, P-value=0.087).
| Perso | ns | Eyes | ||||
|---|---|---|---|---|---|---|
| Medical department | Yes | No | Total | Yes | No | Total |
Surgery |
4 |
6 |
10 |
4 |
16 |
20 |
Internal medicine |
6 |
4 |
10 |
10 |
10 |
20 |
Geriatrics |
3 |
7 |
10 |
4 |
16 |
20 |
Orthopedics |
3 |
7 |
10 |
4 |
16 |
20 |
ICU |
3 |
7 |
10 |
5 |
15 |
20 |
Health professionals (total) |
19 |
31 |
50 |
27 |
73 |
100 |
Control group |
11 |
19 |
30 |
20 |
40 |
60 |
Table 2: Positive findings of bacteria presence in five medical departments - surgery, internal medicine, geriatrics, orthopedics, and ICU. The two bottom rows show the total health professionals (from all departments) and the control group. Both eyes of each participant were tested, leading to the double number of eyes. A positive finding indicates the presence of bacteria in the eye, and a negative finding indicates a sterile sample.
Significant differences of the Internal medicine department with Geriatrics and Orthopedics, no significant difference in bacteria incidence was found between any other two departments as shown in table 3 that shows P-values of comparisons between the various departments and the control group using Fisher’s exact test. Values lower than 0.05 are marked and imply significant difference in bacteria incidence between the two corresponding departments, as discussed above.
| Fisher’s exact text P-values | ||||||
|---|---|---|---|---|---|---|
| Surgery | InternalMedicine | Geriatrics | Orthopedics | ICU | Control group | |
Surgery |
- |
0.038 |
0.305 |
0.305 |
0.275 |
0.125 |
Internal Medicine |
0.038 |
- |
0.038 |
0.038 |
0.071 |
0.087 |
Geriatrics |
0.305 |
0.038 |
- |
0.305 |
0.275 |
0.125 |
Orthopedics |
0.305 |
0.038 |
0.305 |
- |
0.275 |
0.125 |
Intensive Care Unit |
0.275 |
0.071 |
0.275 |
0.275 |
- |
0.179 |
Control group |
0.125 |
0.087 |
0.125 |
0.125 |
0.179 |
- |
Table 3:Fisher’s exact test P-values, comparing bacteria incidence between various medical departments and a control group. This table was created according to the findings presented in Exhibit 2. The P-values represent bacteria incidence in the two corresponding medical departments according to Fisher’s exact test. P-value<0.05 was considered statistically significant (cells marked in gray). Significant differences were found only for comparisons of the internal medicine department with the surgery, geriatrics, and orthopedics departments. All values are shown twice, for convenience purposes only.
Figure 1 shows specific bacteria incidence in each department and in the control group [Only in figure 1b]. As can be seen, the internal medicine department showed a wider variety of bacteria species, which included all four types of bacteria that were found in the control group. Only one type of bacteria (coagulase-negative Staphylococcus) was found in the geriatrics, orthopedics and ICU departments; whereas in surgery, two types were found (Staphylococcus aureus in addition to coagulase-negative Staphylococcus).
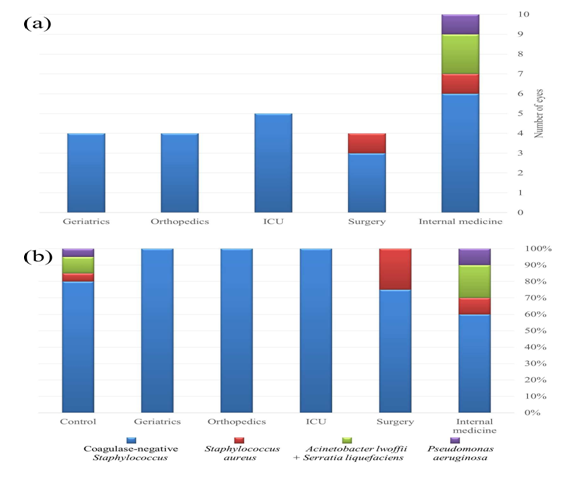
Figure 1:Incidences of bacteria found according to medical department. (a) The number of eyes infected eyes with each bacteria and (b) The percentages of each bacteria of the total bacteria found in the specific groups, in five medical departments and the control group. The legend at the bottom of the figure indicates the types of bacteria.
In this work, we compared the microbial flora of the conjunctiva of health professionals with that of a control group from the general population. We found no significant difference in bacteria incidence or type between these two populations. This does not support our research hypothesis that continuous exposure to the hospital environment affects the normal microbial flora of the conjunctiva. Our assumption was that if a significant difference in the microbial flora of health professionals would be found, an appropriate prophylactic treatment could be initiated in future cases, for the prevention of serious and even irreversible damage. An example of such would be a health professional with an acute or chronic illness or undertaking surgery or other medical procedures.Coagulase- negative Staphylococcus was by far the most common bacteria found in the conjunctiva in the current study. Staphylococcus aureus and gram-negative bacteria presented at much lower, but similar incidences. These findings concur with published studies of healthy individuals [9], though other studies of healthy adults reported Corynebacterium [18] and Staphylococcus epidermidis[14] as the most common bacteria in the conjunctiva. The low diversity found in the current study concurs with the conclusion of an investigation of 107 healthy adults that the healthy ocular surface microbiome is paucibacterial [21], with flora that are distinct from the skin.
Interesting results arise from comparing the microbial flora of the conjunctiva of health professionals in different hospital departments. Bacteria incidence for medical staff in the internal medicine department differed significantly from those of other departments (surgery, orthopedics, and geriatrics). We also found greater diversity in the bacteria in the eyes of the internal medicine department staff. These findings imply a higher level of eye contamination in the internal medicine department and warrant further investigation. However, these results should be interpreted with caution for several reasons. First, our sample size comprised only 10 health professionals from each department and is not large enough to derive unequivocal conclusions. Second, all participants work at the same internal medicine department. Conceivably, hygiene protocols may not be followed rigorously in this specific department, compared to other internal medicine departments. To draw definitive conclusions, multi-center research is needed that will compare between various departments in several medical facilities.
This study has several limitations. First, the possibility of selection bias arises due to the voluntary basis of the participants. Second, we did not differentiate between health professional positions, which may affect the results since each role entails different contact with patients and contaminated environments. Third, since hygiene protocols and their implementation may differ between medical facilities, the results are not necessarily generalizable to other facilities, in other regions of Israel or the world.
An interesting follow-up study would be to re-examine the microbial flora of the conjunctiva for the same participants in this research after a period of time. This could inform regarding the retention of changes in microbe colonies due to recurrent contamination from the environment in the eyes of health professionals. Evidence of lesser changes in the flora of health professionals compared to that of the control group would support the retention of environmental changes and also demonstrate effective protection against infection.
Comparison with a control group was a strength of this study. A similar study conducted in Brazil [19]reported changes in the microbial flora of the conjunctiva of health professionals compared to that reported in the literature. However, that study did not compare the incidence of bacteria to that of the general population in Brazil, but only to that reported in the literature. Taken together, that study and the current one support the notion that the normal flora of the conjunctiva among health professionals may vary between regions, and that a control group must always be included for comparison.
The findings of this study did not confirm our hypothesis of alterations in the microbial flora of health professionals with respect to the general population. However, we did find significant difference in the conjunctival flora of health professionals in different medical departments. A multi-center study is needed to confirm our results. In addition, a follow-up study would inform as to whether the recurrent contamination mechanism is responsible for alterations in the conjunctival flora of health professionals.

Citation: Dvora Pikkel. “Exposure of Hospital Staff to Infections: The Effect of the Hospital Environment on the Microbial Flora of the Conjunctiva". Acta Scientific Ophthalmology 4.4 (2021): 56-62
Copyright: © 2021 Dvora Pikkel. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
