Bisant A Labib*
Associate Professor,Department of Optometry,Pennsylvania College of Optometry at Salus University,United States of America
*Corresponding Author:Bisant A Labib, Associate Professor, Department of Optometry, Pennsylvania College of Optometry at Salus University, United States of America.
Received: February 11, 2021; Published: March 06, 2021;
Introduction:Central serous chorioretinopathy (CSCR) is an idiopathic and self-limiting condition manifesting as one or more serous detachments of the neurosensory retina. It typically occurs unilaterally and in the macular region, with most cases resolving spontaneously. Besides clinical examination, many supplementary tools can be utilized in confirming the diagnosis of CSCR, such as fluorescein angiography (FA), indocyanine green angiography (ICGA), and optical coherence tomography (OCT). The exact mechanism is unknown, but corticosteroids have been suggested to play a role in the pathogenesis of CSCR. This case report describes inhaled corticosteroid use as the cause of CSCR.
CaseReport:A 43-year-old Caucasian female reports with subjective visual blur in her left eye only for several weeks in correspondence with use of a nasal spray. Despite good measured visual acuity, a mildly elevated macular appearance was suspected on fundus examination. OCT testing confirmed these findings and elucidated a diagnosis of central serous chorioretinopathy. Resolution with observation and discontinued use of inhaled corticosteroids was achieved.
Discussion:TheOCTisahelpfulandnon-invasivetoolintheassessmentofmacularchanges,dueinthiscase to CSCR. It appears as a serous detachment of the neurosensory retina in the macular region, and often with accompanying pigment epithelial detachment (PED). Complications are rare, but may include OCT findings of choroidal neovascular membrane (CNVM) formation, warranting prompt referral and treatment. The cause of CSCR is multifactorial and not yet well understood. Among other factors, corticosteroids are associated withCSCR.
Conclusion:Most cases of CSCR are self-limiting and resolve spontaneously without treatment, yielding a generally good visual prognosis. Since observation is the most common management approach for acute CSCR, serial OCT testing at initial examination and follow-ups are imperative in monitoring the improvement or worsening of condition. In those worsening or even persistent cases, referral for treatment must be considered to reduce the risk of permanent macular changes and irreversible vision loss.
Keywords: Central Serous Chorioretinopathy; Corticosteroids; Optical Coherence Tomography
Central serous chorioretinopathy (CSCR) is a condition characterized by serous neurosensory detachment of the macula, often accompanied by retinal pigmented epithelium detachment (PED) in approximately 63% of cases[1,2]. This is often a unilateral manifestation, though bilateral cases also may occur. While the serous detachment is primarily confined to the macular region, few cases involve multifocal detachments or extension to the inferior retina[2].
CSCR is typically classified as being acute or chronic. Chronic cases last greater than six months, while acute cases resolve sooner[3]. It is also sometimes classified by some clinicians based on resolution, where acute cases are referred to as those cases in which vision is restored on initial treatment, or chronic if refractory to treatment[4].
The pathogenesis of CSCR is not fully understood and thought to be idiopathic and multifactorial[1]. However, several associations and risk factors have been documented, as this condition often affects middle-aged men much more than women, and patients with a type A personality or high affinity for stress[3-5]. Other associations involve the use of pharmacological agents, such as corticosteroids and sympathomimetic drugs, and a history of infection with Heliobacter pylori[3,5,6]. One case postulates a rare association with CSCR and blunt trauma[7].
The quantity of serous accumulation and precise location of the fluid is what accounts for the symptoms experienced in patients with CSCR. If central in location, patients may report decreased vision, distorted vision, reduced contrast sensitivity, and altered color vision[4]. These patients may also have central or paracentral relative scotomas on visual field testing[8]. If fluid is located outside of the macula, patients may often be asymptomatic[4].
A unique feature of this case is the patient’s lack of visual acuity reduction in the affected eye despite central serous fluid accumulation. This can be best explained through studies evaluating the effect of luminance levels on patients with CSCR. Patients will often have an easier time with daytime activities, where luminance is higher, than evening activities where luminance is low.
This correlates with high luminance visual acuity charts and may falsely over estimate vision in these patients[8].
A 43-year-old Caucasian female reported to the primary care clinic with chief complaint of very mild, gradual blur in her left eye for approximately five weeks. The timing of the blur was described as constant at distance and near, and she reported that it has marginally improved within the last couple of days. She denied any additional complaints, such as flashes, floaters, diplopia, redness, discomfort, or new headaches. She could not recall the location or specific time frame of her last eye examination, as it was several years ago. However, she reported that she did have a pair of spectacles from that visit which she wore full time. She denied any history of ocular diseases ortrauma.
Her medical history consisted of seasonal allergies and nasal congestion, for which she recently began use with Flonase nasal spray (fluticasone propionate, Philadelphia PA) once daily for the last month. She denied the use of additional medications or any medication allergies. She also denied hypertension or diabetes mellitus. Her family history was positive for diabetes mellitus and hypertension (father). She was not pregnant or nursing at that time. Her social history was significant for drinking a glass of wine on occasion and she had no history of cigarette use.
Entering visual acuity without correction was measured at 20/50-2 in the right eye and 20/50+2 in the left eye at distance and 0.4/0.6M in the right and left eye at near. With the use of her habitual glasses, her acuity improved to 20/15-2 in the right eye and 20/20 in the left eye at distance. Her near acuities also improved to 0.4/0.4M in the right eye and 0.4/0.5M in the left eye. Cover test revealed an orthophoric position at distance and near. Pupils were equal, round, and reactive to light with no afferent pupillary defect in either eye. Extraocular muscles displayed full range of motion in both eyes and Hirschberg reflexes were symmetric. Confrontation visual fields were fulltofingercountingintherightandlefteyes.Amslertestingwasperformedwithherhabitualspectacles in response to her chief complaint, which did not reveal scotomata or metamorphopsia in either eye.
Lensometry on her habitual glasses measured a prescription of -1.00-2.00x132 in the right eye and plano-2.25x060 in the left eye with a +1.25 additional power at near. Subjective refraction at that visit was performed, with her final prescription -0.50-2.00x130 in the right eye and +0.50- 2.50x060 in the left eye. The additional power at near remained the same, at +1.25 with a range of clear vision at near from 10 cm to armslength.
Slit lamp examination of the anterior segment revealed clear lids and eyelashes in each eye. The bulbar conjunctiva in both eyes were white and quiet, and palpebral conjunctiva were pink and quiet. The cornea was clear with no surface abnormalities or staining in either eye. Her anterior chambers were deep and quiet, with a grade 4 Van Herrick in each eye. The irises were flat and intact, and hazel in color in each eye. Intraocular pressures measured 16mmHg in each eye using Goldmann applanation tonometry (GAT). Blood pressure was measured in office at 122/76 mmHg, right arm sitting. The patient was then dilated with a drop of 1% tropicamide and a drop of 2.5% phenylephrine.
Dilated examination was performed with a 90D lens and binocular indirect ophthalmoscopy. The lens and vitreous was clear and intact in each eye. The peripheral and mid-peripheral retina in each eye was flat and intact, with no breaks or detachments 360. Optic discs were healthy and perfused with distinct margins in both eyes. The cup-to-disc ratios in the right and left eyes were recorded as 0.25/0.25 with no apparent nerve fiber layer dropout. Blood vessels in both eyes followed a normal course and caliber. The macula in the right eye was flat and intact with the presence of a foveal reflex. The macula of the left eye was mildly elevated, with no foveal reflexpresent. Due to the changes in macular appearance in the left eye, an OCT was performed revealing central serous chorioretinopathy.
(Figure 1 and 2)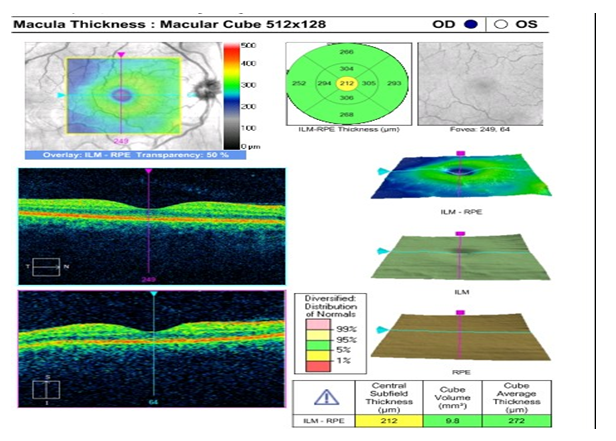
Figure 1:OCT OD revealing normal foveal contour and no breaks or detachments.

Figure 2:OCT OS revealing serous macular detachment.
The patient was then educated on the examination findings and possible correlation of fluticasone and other steroidal use with the findings in her left eye. She denied recent stress, infection, or autoimmune disease. She reported that she was employed as a full time middle school teacher, which she did not describe as an overly stressful position. She was given an Amsler grid for home monitoring to use 2-3 times per week until her next follow up in 6 weeks to re-assess retinal status. She understood that she needed to return as soon as possible if any changes arise on the grid, or if any new ocular or visual complaints are experienced.
Follow up visitThe patient returned six weeks later for follow up, reporting no changes on home monitoring with Amsler grid and resolution of blur that was previously reported at her last visit. There also had been no new changes to her systemic or ocular health. She had reduced the use of her fluticasone nasal spray to once per week following discussion of possible correlation between CSCR and steroid use.
Her entering, aided visual acuities at distance were 20/15-2 in the right eye and 20/15-3 in the left eye. Pupils were equal, round, and reactive to light with no afferent defect in either eye.
Extraocular muscles were full in each eye with symmetric Hirschberg reflexes. Confrontation fields were full to finger counting in each eye.
Slit lamp examination revealed clear lids, lashes, conjunctiva, and corneas in the right and left eyes. Irises were flat and intact and anterior chambers were deep and quiet. Her intraocular pressure was measured at 15 mmHg in the right eye and 16 mmHg in the left eye, using GAT. Her blood pressure at that visit measured 120/80-mmHg right arm sitting and she was again dilated with 1% tropicamide and 2.5% phenylephrine.
Dilated examination remained unchanged from her previous visit, with the exception of her left macula, which then appeared flat and intact. OCT was performed for comparison, revealing normal foveal contour in each eye and full resolution of CSCR. The right eye remained stable (not pictured).
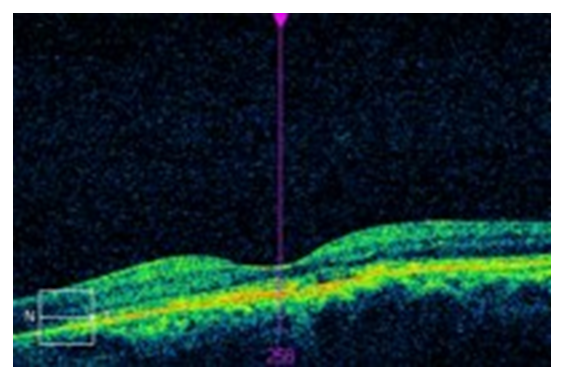
Figure 3:OCT OS on 6 week follow up portraying full recovery from CSCR.
The pathophysiology of CSCR was once thought to occur secondary to RPE dysfunction, as observed on FA[1,2]. The reason for the dysfunction is unknown, but the impaired RPE cells result in a breakdown of the barriers preventing fluid moving in the chorioretinal direction[9]. However, more recent studies using indocyanine green (ICG) angiography have challenged this theory, where multifocal areas of choroidal vascular permeability secondary to ischemia, stasis, or inflammation were evident, even in the asymptomatic fellow eye[1,10]. It is now suggested that the exudative changes in the choroid are the primary event, followed then by the subsequent RPE dysfunction, which allows the fluid from the choroid to enter the subretinal sensory space to accumulate leading to a neurosensory retinal detachment with or without the presence of PED[1,2].
As we are now aware, the choroid is the primary site of this pathology. In patients with CSCR, increased choroidal thickness has been reported. This variability in size is due to the dilatation of large, hyperpermeable choroidal blood vessels in CSCR patients. Superficial to this thickened layer is an area of medium and smaller sized blood vessels, known as the inner choroidal layer. In regions where there is marked choroidal thickening, the adjacent inner choroidal layer is thinner than normal tissue, due to primary atrophy or direct compression by the underlying dilated vessels. This direct compression and resultant mechanical stress can also lead to reduced RPE adhesion, alteration of RPE hydro-ionic regulation, and RPE atrophy. A combination of these events will ultimately manifest clinically as a PED[11]. The dysfunctional RPE is also the site of vascular endothelial growth factor (VEGF) and interleukin-6 (IL-6) release, further promoting vascular permeability and exacerbating CSCR[12].
Familial cases of CSCR have been reported, suggesting a possible genetic predisposition. Studies have explored the link between complement factor H (CFH) and CSCR, suggesting that there is an association[11]. CFH is produced by both the choroidal and RPE cells and is important in controlling local intraocular inflammation through the downregulation of the alternative complement pathway[13].
An imbalance in sympathetic and parasympathetic stimulation has also been observed in patients with CSCR, demonstrating over activation of sympathetic pathways and decreased parasympathetic activity. This can aid in the explanation of the variability in choroidal blood flow, as it is under the control of the autonomicnervoussystem.Studies have also demonstrated direct damage and apoptosis to RPE cells induced by epinephrineadministration[11].
A psychopathological association has been made regarding the incidence of CSCR to patients with type A personalities. These personal characteristics did not appear to be evident in the patient in the aforementioned case, but include traits such as an aggressive, uncooperative, highly stressed or hostile nature[11]. It is important to note that Helicobacter pylori (H. pylori) gastrointestinal infections are also associated with both type A personalities and the development of CSCR[14]. The link between high stress personalities and CSCR has yet to be fully understood, but may implicate the elevated cortisol levels in these patients. Pregnant patients and those with Cushing syndrome also exhibit higher cortisol levels, and a subsequent elevated risk of developing CSCR[11].
Other hormonal factors have also been suggested in the pathophysiology of CSCR, as there is a strong association between it and elevated glucocorticosteroids and catecholamine levels[1,10]. This is an important theory to consider, since the patient presented in this case was being treated for nasal congestion with glucocorticosteroids.Glucocorticosteroid use causing increased levels in the body may have an effect on the permeability of the choroid, RPE, and Bruch’s membrane. As it pertains to the choroid, the increased expression of adrenergic receptors may induce vascular autoregulation. Corticosteroids are also known to affect water and ion transport, which may increase the permeability of the RPE[10]. Finally, corticosteroids inhibit fibroblastic activity and collagen synthesis. Suppression of such activity affects Bruch’s membrane, which is primarily composed of collagen. This leads to decreased choroidal repair and persistent leakage[15].
DiagnosisDiagnosis of CSCR occurs through the evaluation of clinical signs and symptoms as were previously discussed. In addition to a thorough history and examination, FA can also be used. Characteristically, CSCR would appear as focal single or multiple leaks from the RPE and choroid[2]. Early in the disease, a focal area of hyperfluorescence near the fovea is observed, secondary to the seepage of dye from the choroid through the RPE. The dye is then spread to more diffuse locations, typically in an inkblot or mushroom-shaped pattern. The smoke stack pattern is also possible, though much less common. Previous episodes of CSCR can be evident as RPE window defects or the presence of capillary dropout and telangiectasia in the retinal layers[16].
ICG angiography shows additional choroidal vascular permeability, which has alluded to the choroid as the primary area of disease pathology[1,16]. Initially, there is hypofluorescence representing a delay in arterial filling, followed by hyperfluorescence from choroidal hyperpermeability, and finally the washout of the ICG dye[16].
The use of OCT in the diagnosis and management of CSCR is beneficial in that it is a more readily available and less invasive modality than FA or angiography. In subtle cases where visionis mildly affected and the presence of subretinal fluid can be inconspicuous, the OCT will clearly reflect pathological changes[16]. Diagnostic characteristics on OCT include neurosensory retinal detachment, PED, fibrinous exudates, and cystic retinal changes[1]. More importantly, the OCT has been able to measure the thickness of the choroid, which is the main structure implicated in the CSCR, exhibiting a greater thickness in affected eyes[10]. PEDs are more readily observed using OCT than in more invasive techniques utilizing angiography[16]. More recent studies evaluated the appearance of specific retinal layers in CSCR, demonstrating that the photoreceptor (PR) outer segments are often thickening during the course of the disease, and display a granular appearance on imaging. The granular appearance is likely secondary to the accumulation of the discs that are shed[1]. Thickness of the outer nuclear layer was shown to correlate with visual acuity, as well as the reduced distance from the internal limiting membrane to the external limiting membrane[10].
The OCT is also helpful in monitoring the course of CSCR. In cases as presented here, the OCT was essential in the diagnosis and resolution of condition, as the patient was only mildly symptomatic and visual acuity generally unaffected. In cases where CSCR is treated, OCT is helpful in determining the effect of the treatment. Due to its ability to measure choroidal thickness, a 20% reduction in thickness has been detected in successful photodynamic therapy (PDT)[10].
Treatment80% of CSCR cases resolve spontaneously without complication in 3-4 months, making observation the first line approach in treatment[1]. In relevant cases, risk factors should be addressed in addition to monitoring, such as the use of glucocorticosteroids or lifestyle changes to aid in coping with stress[5]. Chronic cases should be evaluated for treatment to prevent complications and permanent visual reduction, though there is currently no gold standard treatment approach for CSCR[16].
The patient in this case was counseled on the disuse of intranasal corticosteroids and observed until full resolution 6 weeks later. Pascual.,et al. reported a series of three cases where patients on systemic steroids for rheumatologic conditions were tapered and exhibited complete resolution of CSCR without treatment[17]. Another case, describing the first report of intranasal steroid use and resultant CSCR, discussed the complete and spontaneous resolution 8 weeks later with discontinued use of intranasal steroid use[18].
In the less common persisting cases, anti-VEGF agents were attempted as treatment due to the hypothesis that choroidal hyperpermeability is associated with increased VEGF expression.
However, little improvement was evident in clinical trials. It is better considered in complicated cases of CSCR, where CNVM formation occurs and can thus be treated with these injections[5].
Laser photocoagulation, in the form of argon laser or micropulse diode laser, is a possible treatment option that allows the acceleration of the absorption of subretinal fluid in persisting cases of CSCR. Micropulse lasers have also been thought to directly affect leakage of the RPE[4].
Veterporfin PDT is beneficial in the treatment in CSCR as well as the prevention of recurrences in some cases. It has been speculated that treatment immediately reduces the permeability of choriocapillaries and, later on, leads to long term vascular remodeling and resultant hypoperfusion and leakage prevention[4]. Studies evaluating half-dose veterporfin PDT showed that it was as effective and safer than the full dose[19].
The presentation of CSCR in this case is unique because it occurred in a female patient with no measured visual decline on examination. In other ways, it is characteristic of CSCR, such as the findings of serous detachment on OCT, use of steroids, and spontaneous resolution without treatment. It highlights the importance of the pathogenesis of CSCR and its relationship with steroid use, an advisory point of patient educated and co-management with physicians who place patients on steroidals. The OCT was essential in this case to monitor the resolution of disease on follow up.

Citation: Bisant A Labib., “Inhaled Corticosteroid Use and Central Serous Chorioretinopathy". Acta Scientific Ophthalmology 4.4 (2021): 10-16.
Copyright: © 2021 Bisant A Labib., This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
