Camara MLT*, Bangoura S, Traore A, Traore M, Barry KMB, Diallo AY, Diallo Mm, Bah AO, Kaba ML
Donka Nephrology-Haemodialysis Department, UGANC, Guinea
*Corresponding Author: Camara MLT, Donka Nephrology-Haemodialysis Department, UGANC, Guinea.
Received: December 13, 2024; Published: December 29, 2024
Citation: Camara MLT., et al. “Circumstances of Initiation of Hemodialysis: Value of Early Nephrological Follow-Up". Acta Scientific Paediatrics 8.1 (2025): 16-21.
Introduction: Chronic renal failure is a major public health problem, with a steadily rising incidence. The aim of this study was to assess the circumstances surrounding the initiation of haemodialysis in terms of the value of early nephrological follow-up.
Material and Methods: This is a prospective descriptive and analytical study lasting 3 months, from 1er September to 30 November 2022, in the context of chronic renal failure in patients who were followed up early before being put on chronic haemodialysis, and groups of chronic haemodialysis patients in a late context in the adult haemodialysis centre.
Results: Out of a total of 78 patients initiated on haemodialysis, we included 70 patients in the study. 13 patients were in early nephrological follow-up, i.e. 16.67%, and 57 patients were in late nephrological follow-up, i.e. 73.07%. The mean age of the patients was 46.43 ± 14 years, and the main indication for initiation of haemodialysis was uraemic intoxication in 52 cases (74.29%). Early initiation of haemodialysis was observed in 13 patients, with favourable outcomes in 13 and zero deaths; late initiation in 57 patients resulted in 4 deaths.
Conclusion: The ideal time to initiate dialysis in patients with end-stage chronic kidney disease remains a matter of debate. Interdisciplinary collaboration could encourage early referral at the stage of onset of chronic kidney disease, thereby improving the quality of haemodialysis.
Keywords: Initiation; Haemodialysis; Nephrological Follow-up
Chronic renal failure is a major public health problem, with the incidence of the disease rising steadily. Patients are referred to nephrologists at a late stage [1].
Emergency haemodialysis is very common in nephrology, and is associated with a high morbidity and mortality rate [2]. The ideal time to initiate dialysis in patients at the stage of CKD remains a matter of debate. There is conflicting evidence in the literature as to the benefit of early initiation of renal replacement therapy [3].
In 2016, around 50,000 patients in France were living on dialysis. The decision to start dialysis is a multifactorial one. They affect both the patient and the healthcare team [4]. In the end-stage of chronic kidney disease, patients need a long-term replacement method, such as extra-renal purification (peritoneal dialysis or haemodialysis) or kidney transplantation [5]. Conservative treatment, which in some cases is increasingly seen as a treatment option in its own right, helps to alleviate the complications of chronic renal failure through symptomatic management [5]. For patients with CKD, dialysis was started as an emergency treatment for 32% of them [6].
The true extent of the ́IR in sub-Saharan Africa remains unknown due to a lack of national registries [7].
In 2005, end-stage renal disease was a major public health concern in Morocco. Its incidence is 162 new patients per million inhabitants [8].
In Tunisia in 2017 at Charles-Nicolle Hospital, in Medicine Department A, out of 229 patients who started HD. Only 132 patients (57.6%) were referred early to the nephrologist [1].
In Togo in 2019, a hospital frequency of 93.7% of patients had end-stage chronic renal failure, ́haemodialysis is the basis of management [7].
In 2020 in Senegal, out of 263 patients, 107 underwent emergency dialysis, representing a prevalence of 40.68%. The emergency department of the Thiès regional hospital was the main referral facility with 27.1%, and 23 patients (21.06%) had a known kidney disease before the first emergency dialysis session [2].
Given the absence of previous studies on this subject in our country, we thought it would be useful to carry out this study, the aim of which was to assess the circumstances surrounding the initiation of haemodialysis from the angle of the value of early nephrological follow-up.
This is a prospective descriptive and analytical study lasting 3 months, from 1er September to 30 November 2022, in the context of chronic renal failure in patients who were followed up early before being put on chronic haemodialysis, and groups of chronic haemodialysis patients in a late context in the adult haemodialysis centre.
Guinea has just one public haemodialysis centre, located in the Donka University Hospital. It is a referral service for kidney disease.
We targeted a population of chronic haemodialysis patients in two groups, the first consisting of patients with CKD who had benefited from early nephrological follow-up before being placed on haemodialysis, and the second group consisting of patients with CKD who had benefited from late haemodialysis.
The study population consisted of chronic haemodialysis patients who were hospitalised or followed up on an outpatient basis during the study period.
Our study included
Exhaustive recruitment of all haemodialysis patients meeting our selection criteria during the study period. We used the sample size calculation formula and obtained a sample equal to 70 patients, the data being collected on individual survey forms.
The variables were: frequency, age, sex, general condition at initiation of HD, indication for haemodialysis at initiation, nephrological follow-up, treatments and progression.
Each variable was defined to describe the measurement methods:
We used an anonymous questionnaire, a survey form and a data collection tool. The questionnaire was submitted to the respondents with their informed consent.
The data on the survey form were entered and analysed using Epi-info software version 7.2.3.1. Word and Excel software from the 2019 Office Pack were used to enter the document and present the results in the form of tables and figures.
Qualitative variables were expressed as proportions and quantitative variables as means ± standard deviation. The Chi-square test and Fisher's exact test were used to compare proportions, and the Student's t test was used to compare means. Statistical significance was considered when the P value was less than 0.05.
Nephrological follow-up rate: out of a total of 78 patients initiated on haemodialysis, we included 70 patients in the study, 13 patients (16.67%) with early nephrological follow-up and 57 patients (73.07%) with late nephrological follow-up.

Table 1: Distribution according to nephrological follow-up rate of the 70 CKD patients initiated on haemodialysis during the study period.
Age: Our patients were divided into age groups with a range of 10 years. Out of a total of 70 patients, the 50-70 age group was the most representative in 19 cases, i.e. 27.15%. The mean age of the patients was 46.43 ± 14 years, with extremes of 17 and 75 years (Table 2).
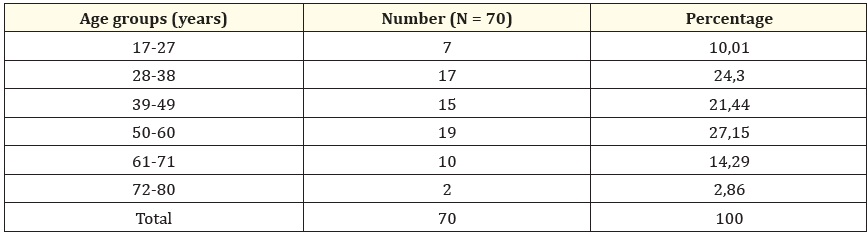
Table 2: Age distribution of 70 CKD patients initiated on haemodialysis during the study period. Mean age: 46.43 ± 14.70 years Extremes: 17 years and 75 years.
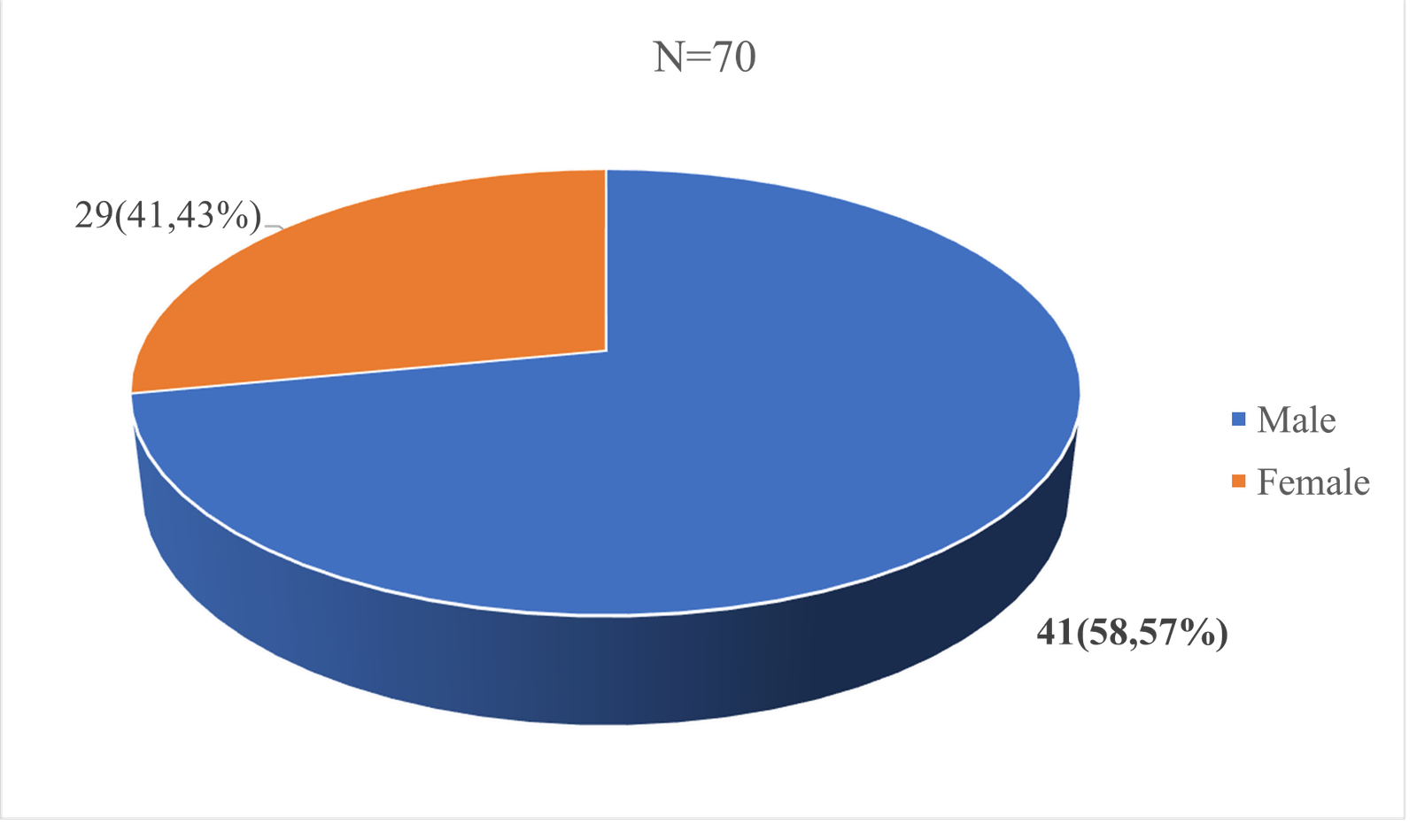
Figure 1: Out of 70 patients, the male sex was representative in 41 cases, i.e. 58.57%, and the female sex was representative in 29 cases, i.e. 41.43%. We observe a male predominance, with a sex ratio of 1.41. Sex ratio = 1.41.
Out of 70 patients with chronic renal insufficiency initiated on haemodialysis, 33 cases (47.14%) had an altered general state and 8 cases (11.43%) were in a coma, requiring emergency haemodialysis (Table 3).

Table 3: Distribution according to general condition of the 70 CKD patients initiated on haemodialysis during the study period.
Of 70 patients with chronic renal failure initiated on haemodialysis, the main indication for initiation of haemodialysis was uraemic intoxication in 52 cases (74.29%).
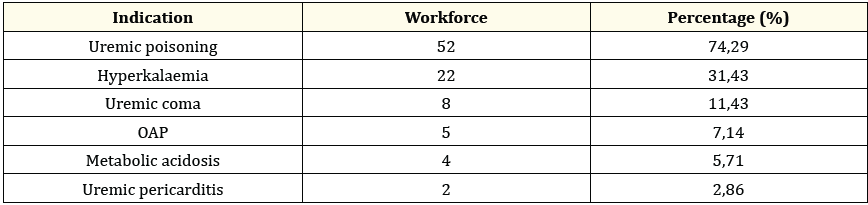
Table 4: Distribution according to HD indication of the 70 CKD patients initiated on haemodialysis during the study period.
Out of 78 patients with chronic kidney disease during the study period, haemodialysis was initiated in 70 patients (89.74%) and 8 patients (10.26%) opted for conservative treatment.

Table 5: Breakdown of patients by treatment method.
Of 70 patients with chronic renal failure initiated on haemodialysis, early initiation occurred in 13 patients and late initiation in 57 patients. We noted 4 cases of death.
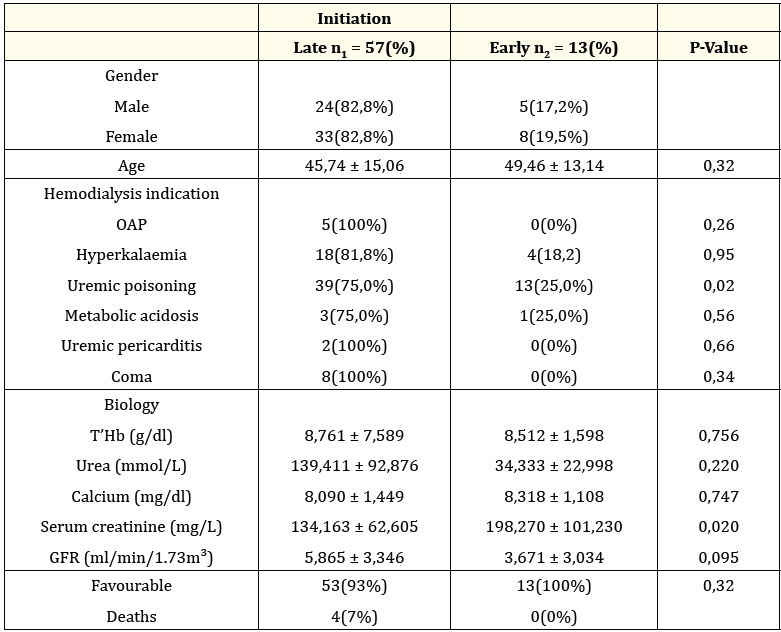
Table 6: Comparison of data between monitored and unmonitored CKD patients initiated on haemodialysis during the study period.
The aim of this study was to assess the impact of early nephrological follow-up compared with late referral of patients with end-stage renal disease to nephrology, and to understand the impact of late referral on the lives of patients on chronic haemodialysis.
Of 70 patients with end-stage chronic kidney disease for whom haemodialysis was initiated, 13 patients (16.67%) had early nephrological follow-up, compared with 57 patients (73.07%) with late nephrological follow-up.
These proportions would explain why the majority of patients with chronic end-stage renal disease are discovered late, and late initiation of haemodialysis could be a factor that maintains mortality in haemodialysis.
The potential limitations of the study were the reluctance of patients to start haemodialysis because of low financial means, which had an impact on the number included in the study, and could influence the internal and external validity of the results. We compared our data with the current scientific literature:
Out of 70 patients with end-stage renal disease, uraemic intoxication was the main reason for initiation of haemodialysis in 52 cases (74.29%). This proportion indicates a high complication rate and a delay in starting haemodialysis, which may be factors in haemodialysis mortality.
In this study, comparing the late indication for haemodialysis with the early indication, we observed a favourable outcome in 13 cases (100%) of early nephrological follow-up, with death occurring in around 4 cases (7%) of patients referred late.
SAAD Benali in 2016 in Rabat in thesis N°198 from the Faculty of Medicine, concerning the value of early monitoring of chronic renal failure patients before renal replacement therapy in 318 cases, RT is responsible for poorer control of the consequences of chronic uraemia [8].
Eyéni Sinomono D., et al. in 2018 in the nephrology department of Brazzaville, concerning the initiation of dialysis, out of 244 patients identified, the decision to start haemodialysis was based on GFR and urea levels in 9% of cases [3].
Felah., et al. in 2018 in Tunisia at the charles-Nicolle hospital, in the nephrology department, out of a total of 115 patients, emergency haemodialysis was undertaken for threatening hyperkalaemia in 47.8% of cases, acute lung oedema in 33% of cases, severe metabolic acidosis in 18.2% of cases. Death occurred in 3% of cases [2].
Our results have internal validity based on the practical modalities of the variables measured on the one hand, and on the results obtained in comparison with data in the scientific literature on the other. The presence of a bias due to the size of the sample, which is smaller than that of other studies, influences the external validity of our study, but the results are usable in our local context.
In the future, this study will enable us to broaden the level of screening for chronic kidney disease and improve interdisciplinary collaboration to encourage early referral of chronic kidney disease to nephrologists in order to prepare for high-quality haemodialysis in order to improve the survival of haemodialysis patients.
In the field, the informed consent of the participants was obtained before submitting them to the questionnaire and strict confidentiality was respected.
During the course of our work, our difficulties were the lack of financial resources and the reluctance to start extra-renal purification.
The ideal time to initiate dialysis in patients with end-stage chronic kidney disease remains a matter of debate. Patients are referred to nephrologists at a late stage. There is conflicting evidence in the literature about the benefits of early initiation of renal replacement therapy. In our context, patients initiated on haemodialysis account for 16.67% of early nephrological follow-up and 73.07% of late referrals, with 7% of deaths due to late initiation of dialysis. Interdisciplinary collaboration could promote early referral at the stage of early chronic kidney disease, thereby improving the quality of haemodialysis.
All authors participated in data collection, analysis and writing of the manuscript. The manuscript was read and accepted by all authors.
Copyright: © 2025 Camara MLT., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.