Abdulwahab Alijubab1, Ilhama Jafarl2, Majd Hadad3, Alexandra Richards4, Brejeetta John5*, Hadeel Abdulwahab Alshammar6 and Reem Abdulwahab Alshammari7
1 Consultant Paediatric Surgeon, Program Director and Chairman, Riyadh, Saudi Arabia
2 Paediatric Surgery, Chelsea and Westminster Hospital, UK
3 Paediatric Surgery, Children’s Specialised Hospital, King Fahad Medical City, Saudi Arabia
4 Urology, University Sussex Hospital Trust, UK
5 Medicine, Cardiff University, UK
6 Paediatric Critical Care, King Fahad Medical City, Saudi Arabia
7 Senior Registrar Obgyn, Free Agenty, Saudi Arabia
*Corresponding Author: Brejeetta John, Medical Student, Cardiff University, UK.
Received: March 16, 2024; Published: April 23, 2024
Citation: Brejeetta John., et al. “The Prevalence of Paediatric Surgical Diseases, and the Operative Mortality, at a Single Tertiary Centre in Saudi Arabia”. Acta Scientific Paediatrics 7.5 (2024): 06-12.
Background: The burden of surgical diseases in low and middle-income countries (LMICs) is relatively high due to the lack of resources for adequate surgical care. This affliction is significantly higher in the pediatric population as children tend to have more complex surgical needs. This research aims to identify the prevalence of pediatric surgical diseases, the most common paediatric surgical diseases and the operative mortality, at a single tertiary centre in Saudi Arabia. It will also help to identify the outcomes of paediatric surgical diseases which will help to better educate the public about the most common surgical presentations in children.
Methods: A retrospective chart review was conducted at a single surgical centre in King Fahad Medical City in Riyadh over a sevenyear period (2010-2017). All patients younger than 14-years-old at presentation, with pediatric surgical diseases, were included for analysis.
Results: Two hundred and twenty patients have been identified. The majority of patients were from the Riyadh and Al-Qassim region. The male to female ratio was 1:0.94 respectively. The most common diagnosis was Wilms tumour (37.2%) followed by Hirschsprung’s disease (23.3%). In total, 202 (90.6%) patients underwent one operation, with 48.4% and 12.1% undergoing secondary and tertiary procedures respectively. Seventy-eight (36.1%) patients were admitted to intensive care units for rehabilitation and/ or post-surgical care, of which 66.7% were admitted for less than two weeks. There were 37 (16.6%) patients with complications following surgery, of which the majority occurred less than 30 days post- operatively (77.8%). The overall mortality and morbidity rates were 0.9% and 10.3% respectively. Long- term development was normal in 189 (87.5%) patients.
Conclusion: This study demonstrates the spectrum of surgical conditions in a single tertiary hospital in Riyadh, which supports children from all regions of Saudi Arabia. This gives valuable insight outcomes of common pediatric surgical diseases. Based on this data, this article highlights the need for improved education, resource allocation and tailored outreach programmes to support children with a limited access to surgical care. However, we recognize that the small sample size in the study limits generalization of our results to the paediatric population of Saudi Arabia.
Keywords: Urgical Diseas; Paediatric; Prevalence; Restrospective Review
LMIC: Low and Middle-Income Countries; DALYS: DisabilityAdjusted Life Years; KFMC: King Fahad Medical City; ASA: American Society of Anesthesia; CDH: Congenital Diaphragmatic Hernia; WHO: World Health Organisation.
It has been estimated that 5 billion children do not have access to safe and appropriate surgical care around the world. [1,2] Approximately 85% of children with surgical pathologies attribute to the current global burden of disease, with low and middleincome countries (LMIC) bearing the greatest load. [3] Additionally, a recent study published in the Lancet has suggested that 143 million more surgeries are needed to reduce the current morbidity and mortality rates seen in LMICs, of which an estimated mean of 32.9% deaths are attributed to surgical pathology. [2,4] However, despite this growing awareness of the global burden of surgical diseases, there is still little focus on pediatric surgical conditions worldwide. Congenital anomalies and peripartum complications are two of the leading causes of mortality worldwide for children under five years old. These anomalies are liable for 13% of disability-adjusted life years (DALYS) across the globe. [6-8] Therefore, pediatric surgical care should be considered an essential component of child health programs in developing countries. This research aims to identify the prevalence of pediatric surgical diseases, and the operative mortality, at a single tertiary centre in Saudi Arabia.
This retrospective chart review was conducted over a sevenyear period from 2010 to 2017 at a single surgical centre in King Fahad Medical City (KFMC) in Riyadh, Saudi Arabia. KMFC is one of the largest, specialist medical complexes in Saudi Arabia: it comprises of four hospitals treating over 50,000 inpatients and 600,000 outpatients annually. The site has a total capacity of 1200 beds, of which a specialised 253-bed hospital is dedicated to paediatric patients only. All patients younger than 14-years-old at presentation, with pediatric surgical diseases, were included for analysis. Patients were excluded due to age at presentation and if parents/carers signed discharge against medical advice. Emergency surgical procedures due to trauma were also excluded. Data collection was conducted following a predetermined classification system: categorization by mechanism of injury (congenital or acquired); minor surgery or major surgery; specialized surgery; visceral surgery; wound surgery and perioperative outcome. A database was compiled, and patients were categorized by age, indication, type of operation, American Society of Anesthesia (ASA) risk classifications (numbered 1-5) and urgency of intervention. Urgency was stratified into 3 categories: urgent, semi-elective (operation should be performed within the next 48 hours) and elective (non-urgent).
Statistical analyses were performed with SPSS software (Version 22.0; 2020). Continuous variables are presented as median, minimum, and maximum values, and categorical data is presented as a number and percentage. The choice of endpoints was influenced by the type of intervention, indication (prevention, primary or secondary treatment), and conduct in an academic versus community setting.
Two hundred and twenty patients have been identified from 2010-2017 in Saudi Arabia. The majority of patients were from the Riyadh and Al-Qassim region and 88.9% were of Saudi Arabian nationality. The male to female ratio was 1:0.94 respectively. The most common diagnosis was Wilms tumour (37.2%) followed by Hirschsprung’s disease (23.3%) (see Table 1).
In total, 202 (90.6%) patients underwent one operation, with 48.4% and 12.1% undergoing secondary and tertiary procedures respectively. Seventy-eight (36.1%) patients were admitted to intensive care units for rehabilitation and/or post-surgical care, of which 66.7% were admitted for less than two weeks. There were 37 (16.6%) patients with complications following surgery, of which the majority occurred less than 30 days post-operatively (77.8%). The overall mortality and morbidity rates were 0.9% and 10.3% respectively. Long-term development was not delayed in 189 (87.5%) patients.
Nine (4.1%) patients were diagnosed with Esophageal atresia, with or without fistula, and one (0.5%) patient was diagnosed with duodenal atresia (Table 2). The most common gestational age was term (70%; range 37-42 weeks), but three patients were born prematurely (30%; range 22-36 weeks). There were no deaths in this subgroup of patients, however, four (40%) patients had associated morbidities and complications. Long term development was not delayed in 80%.
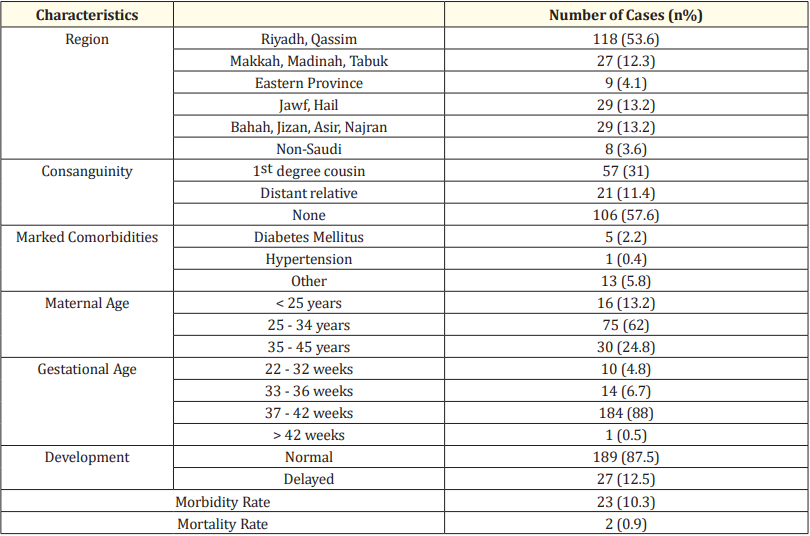
Table 1: Epidemiological data of the entire cohort, between 2010 and 2017 in Saudi Arabia. Numbers are expressed as n (% of cohort).
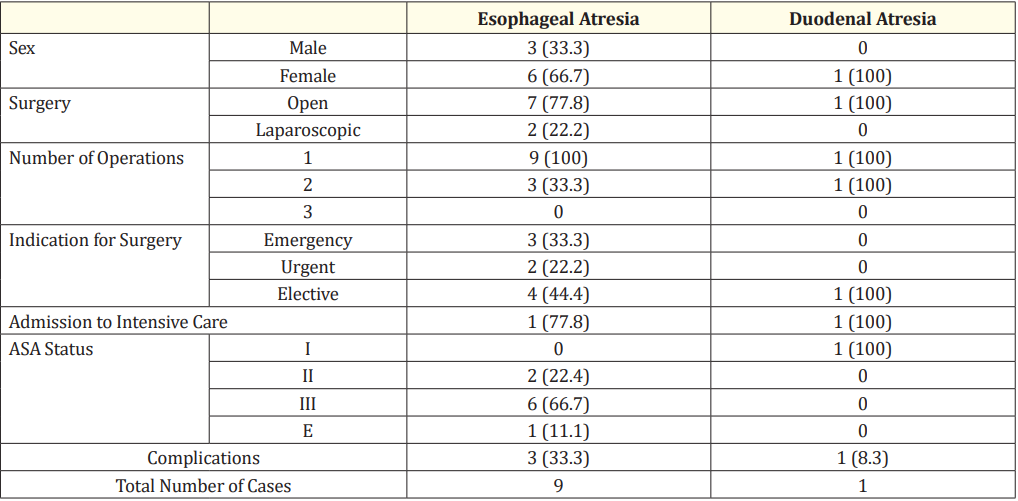
Table 2: Management of upper gastrointestinal surgical diseases. Numbers are expressed as n (% of diagnosis cohort).
Abbreviations: ASA; American Society of Anesthesiologists.
Fifty (23.3%) patients were diagnosed with Hirschsprung’s disease, forty-three (20.0%) patients were diagnosed with anorectal malformation and two (0.9%) patients were diagnosed with malrotations (see Table 3). The most common gestational age was term (83.2%; range 37-42 weeks), but sixteen patients were born prematurely (16.8%; range 22-36 weeks). There were no deaths in this subgroup of patients, however, eleven (11.6%) patients had associated morbidities. Complications occurred in twenty (21.1%) cases. Complications and morbidity rates were highest in patients presenting with Hirschprung’s disease. Long term development was not delayed in 85.3%.
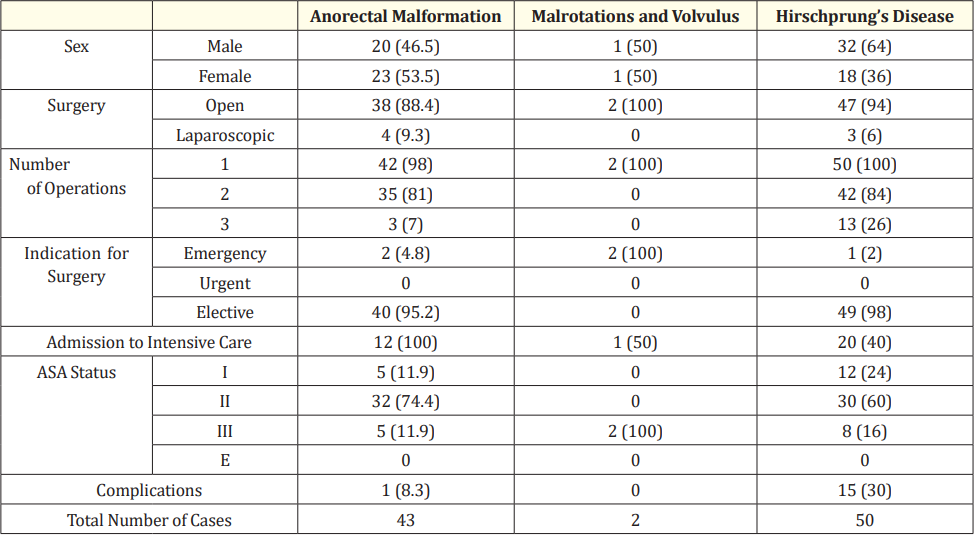
Table 3: Management of lower gastrointestinal surgical diseases. Numbers are expressed as n (% of diagnosis cohort).
Abbreviations: ASA; American Society of Anesthesiologists.
Twelve (5.5%) patients were diagnosed with congenital diaphragmatic hernia (CDH) and two (0.9%) patients were diagnosed with pulmonary sequestration (see Table 4). The most common gestational age was term (85.7%; range 37-42 weeks), but one (7.1%) patient was born prematurely and one (7.1%) patient was born late. There was one death in the CDH group, contributing to an 8.3% mortality rate in the CDH patients identified. Complications and morbidity occurred in one patient each only. Long term development was not delayed in 35.7%.
Eighty (36.4%) patients were diagnosed with Wilm’s tumour and 16 (7.27%) patients were diagnosed with Neuroblastoma. The most common gestational age was term (83.3%; range 37-42 weeks), but three patients were born prematurely (3.1%; range 22-36 weeks). There were no deaths in this subgroup, although 5.2% and 9.4% had associated morbidity and complications respectively. Long term development was not delayed in 93.8%.
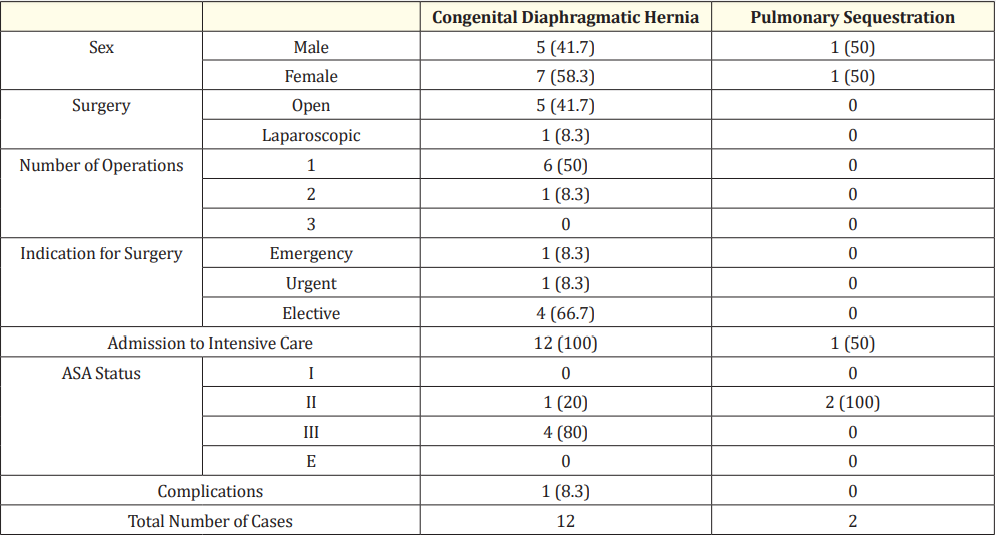
Table 4: Management of thoracic surgical diseases. Numbers are expressed as n (% of diagnosis cohort). Abbreviations: ASA; American Society of Anesthesiologists.
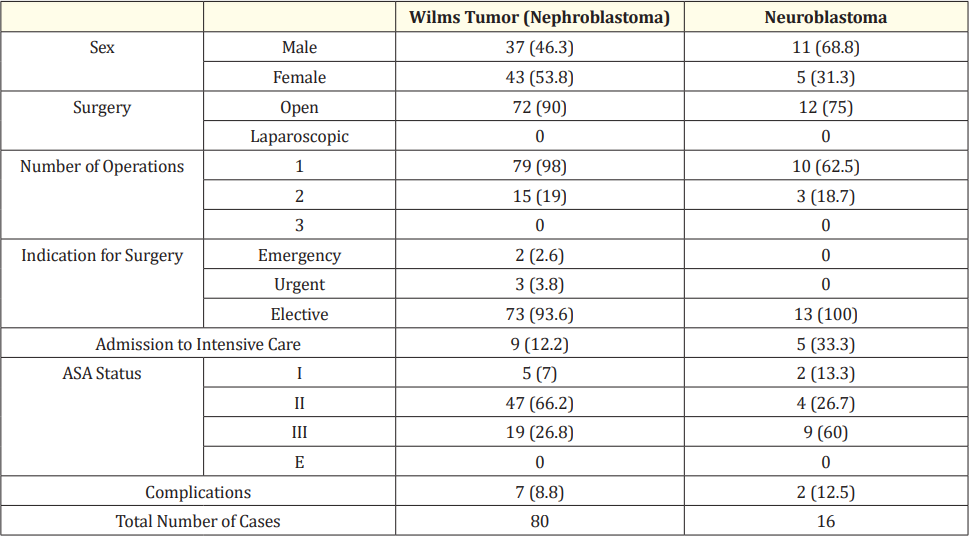
Table 5: Management of malignant surgical diseases. Numbers are expressed as n (% of diagnosis cohort). Abbreviations: ASA: American Society of Anesthesiologists.
The World Health Organisation (WHO) defines ‘Universal Health Coverage’ as the necessary access to healthcare for all individuals and communities, despite financial hardships. [9,10] Following this, the world Health Assembly (WHA68.15) describes the lack of safe surgical care as a ‘global public health issue’ and has recognised the importance of improved surgical resources and accessibility as part of the Universal Health Coverage. [11] Recent estimates have proposed that only 3.5% of pediatric surgical needs are being met, which implies a huge healthcare burden and the need for improved pediatric surgical care to increase the chance of survival in these children. [12] Approaches like structuring training programs, centralization of care and planning for basic surgical services may reduce this burden and improve long-term outcomes. Our research aims to give an estimate of the most common pediatric surgical diseases from a single surgical centre in Saudi Arabia - of which we identified Wilm’s tumour and Hirschsprung’s disease most frequently (36.4% and 22.7% respectively). The highest complication rate was reported in patients with Hirschprung’s disease (30.0%). The highest mortality rate was seen in patients with CDH (8.3%) however, there was only one death in the entire cohort. This data may be used to support public health education for the most common surgical presentations in children, and subsequently improve provisions for these children. However, larger study sizes are needed to corroborate these findings.
The limitations of this study are mainly related to the longterm management because patients do not always return once their surgical procedure is completed. Furthermore, it is difficult to attribute data based on geographic locations where accessibility to surgical care is limited. The lack of such data has made it difficult to define an appropriate role for pediatric surgery in Saudi Arabia, with regards to determining the necessary scope of services, treatment and other aids needed for the management of such patients, as well as assessing the impact of pediatric surgical diseases on, both patient and carer, well-being.
Furthermore, geographical variation in common pediatric surgical conditions and may provide some hints to the etiology of several non-transmissible diseases. [13] This is important to bear in mind with regards to quantifying the need for pediatric surgical specialists, resource distribution and input from multidisciplinary teams. The majority of patients enrolled in this study were from the Riyadh and Al- Qassim region, with patient numbers decreasing as the distance from hospital increased. So, whilst this may support the current literature, it is important to note that these findings are likely an underrepresentation and will not closely reflect the true population of the country. To increase the external validity of these results, larger prospective studies are needed in order to potentially reach those communities and patients who may not have accessible healthcare or surgical services. Further research is needed to establish the true epidemiological data for Saudi Arabia.
This study demonstrates the spectrum of surgical conditions in children in a single tertiary hospital in Riyadh, KFMC, which receives children from all regions of Saudi Arabia. This gives valuable evidence regarding the outcomes of common pediatric surgical diseases. This data may be used to support public health education for the most common surgical presentations in children, and subsequently improve provisions for these children, particularly those with limited access to surgical care.
There were no conflicts of interest or funding opportunities for this article. All authors contributed to production of this manuscript by editing, reviewing, and commenting on previous drafts.
Copyright: © 2024 Brejeetta John., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.