Dias Edwin1* and Dias Anusha2
1Professor and Hod Paediatric Department, Director of Research and Publication Sims and RC, Research Professor Srinivas University Mangalore, India
2Anaesthisiologist and Intensive Care, Father Muller’s Medical College India
*Corresponding Author: Dias Edwin, Professor and Hod Paediatric Department, Director of Research and Publication Sims and RC, Research Professor Srinivas University Mangalore, India.
Received: January 23, 2024; Published: January 30, 2024
Citation: Dias Edwin and Dias Anusha. “Edwin and Anusha’s Technique of Neonatal Reintubation". Acta Scientific Paediatrics 7.2 (2024): 29-30.
Endotracheal intubation is an essential procedure in critical care, allowing life supporting assisted ventilation and providing a conduct through which drugs and devices can reach the lower airways, but it has significant risks whether attempts fail or succeed intubation success, generally defined as placing the endotracheal tube (ETT) within the trachea requires specialized training and the experience of approximately 40 intubations to achieve proficiency. Failed intubation attempts are common particularly in neonatal care where difficult airways are frequent. Patient safety can be compromised during tracheal intubation through failed or prolonged attempts that cause physiologic destabilization, but also through physical trauma, procedure-induced pain and stress, and malposition of the ETT within the tracheal airway, as is the case with deep tracheal or endobronchial intubation.
Inadvertent right mainstem intubation or similar deep malposition of ETT was reported in earlier studies in up to 58% of neonates.in a more recent prospective study on complication of neonatal intubation, the near4neos collaborative reported that mainstem intubations was diagnosed by Xray in 2% of NICU intubations, which is a lower rate than other reports. Using similar methods, the near4kids collaborative, reported mainstem intubation in 13% of inpatients, in our setting. ETT tip beyond the t4 vertebral level was observed in 10.5% of newborns.
All essential equipment is listed and should be available and checked prior commencing the procedure, with individual adaptations appropriate for each baby and clinical setting. Equipment should be set out in a clean and sterile environment where possible in order to minimize contamination.
The patient is fully prepared, monitored and stability maintained while preparations are completed.
Optimise ventilation with high flow, CPAP, Neo puff or bag and mask. Aim to maintain saturations as appropriate for gestation and take care not to hyper oxygenate the preterm infant.
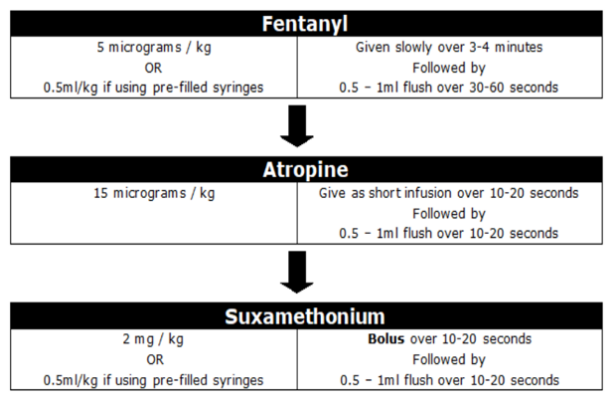
Figure
Copyright: © 2024 Dias Edwin and Dias Anusha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.