Enas Hamdy Elnady1*, Faten Hassan Abdelazium2 and Mostafa El-sherbini3
1Assistant Lecturer, Department of Physical Therapy for Paediatrics, Faculty of Physical Therapy, Cairo University, Egypt
2Professor of Physical Therapy, Department of Physical Therapy for Paediatrics, Faculty of Physical Therapy, Cairo University, Egypt
3Consultant Orthopaedic Surgeon, National Institute of Neuromotor System, Giza, Egypt
*Corresponding Author: Enas Hamdy Elnady, Assistant Lecturer, Department of Physical Therapy for Paediatrics, Faculty of Physical Therapy, Cairo University, Egypt.
Received: January 16, 2024; Published: January 26, 2024
Citation: Enas Hamdy Elnady., et al. “Efficacy of Tilted Seat Surface on Postural Adjustment During Reaching in Sitting Position: In Hemiplegic Cerebral Palsied Children”. Acta Scientific Paediatrics 7.2 (2024): 11-18.
Purpose: The aim of this study to evaluate the effect of seat surface inclination on postural adjustments during forward reaching in sitting position in hemiplegic cerebral palsied children.
Subjects: Fifteen hemiplegic cerebral palsy children aged from 7-9 years participated in this study.
Procedure: During the task of reaching with the affected arm, surface electromyograms were recorded for postural activity and reaching in three conditions: sitting with the seat surface oriented horizontally, sitting with the seat surface tilted 15 degrees forward and 15 degree backward in addition to Modified Functional Paediatric Reaching test.
Results: Backward inclined position associated with more postural activity while in forward inclined seat surface is associated with less postural muscle activity and more forward reaching in terms of modified paediatric functional reach test.
Conclusion: In hemiplegic cerebral palsied children, forward inclination of the seat surface is considered the best position as it is associated with more postural control ability and stability and less postural muscle activity.
Keywords: Seat Inclination; Tilting Seat; Cerebral Palsy Children; Hemiplegia; Postural Control; Postural Adjustment; Reaching; Sitting Position
Cerebral palsy (CP) is one of the causes of physical disability in infants. It is described as a group of permanent disorders that affect the development of movement and posture and attributed to non-progressive disorders in the foetal development or infant brain [1]. It is the most common cause of physical disability in Children with CP have several problems associated with movement and posture includes abnormal muscle tone, activity limitation, lack of equilibrium and alterations in the alignment that affect sitting position [2,3]. Disruptions in sitting postural control significantly affect the development of child, limit the ability to develop balance in sitting position, normal arm, hand functions [4,5] and also the ability to sequence the movements appropriately [6].
Children with CP have problems in adapting the degree of contraction of the postural muscles to the characteristics of the reaching movement and in modulating muscle contraction during reaching to kinematic information on initial body configuration i.e. the sensory information on the sitting position. Thus, postural dysfunction in children with CP would be related to a worse quality of reaching [7].
Tilting of the seat surface are increasingly used by children with disabilities to participate more fully in activities at home and in the community [8], Tilt of the seat may be considered for a variety of reasons, including low sitting tolerance or discomfort, a requirement for efficient relaxed, stable sitting position and assist for functional activities [9].
Appropriate seat positioning of children with motor disabilities is important to achieve maximum function and promote postural alignment and stability. Positioning devices are necessary, in some cases, to prevent undesirable postures that may lead to secondary deformities [10].
A Forward inclined sitting position has been suggested to reduce kyphosis, maintenance of lumbar lordosis as the centre of gravity shifted forward, decreased posterior pelvic tilting on the position of pelvis, reduce the effects of tight hamstring and position a person during reaching on desk or table for more upright and stable sitting posture [11-13].
A backward inclined position makes pressure on the ischia tuberosity [14] or the spine, improves head and trunk posture [15], there are concerns that seating that is excessively tilted backward limits communication, upper limb function and the ability to stand up from chair [16,17].
Electromyography (EMG) recordings have been widely used in the assessment of postural function. EMG amplitude analyses have been extensively used in order to measure the magnitude anticipatory and postural muscle activity with voluntary movements [18]. The amplitude of the EMG signal is an indicator of the magnitude of muscle activity, and is produced by increases in the number of active motor units and the frequency of activation. Naturally, EMG amplitude increases as the intensity of muscle contraction increases. However, the relationship between EMG amplitude and force frequently is nonlinear [19].
Paediatric modified functional reaching test is a highly useful, valid, reliable, quick, simple test used to measure the amount of forward and side reaching with movement of trunk, the test used to reflect the balance, stability and postural control ability during reaching [20,21].
Children with cerebral palsy often hampered by dysfunctional postural control during reaching; it is debatable whether postural control in sitting position during reaching can be enhanced by inclination of the seat surface [22], The aim of our study to determine the effect of seat inclination on postural control during reaching and which sitting position can be considered the best for hemiplegic cerebral palsied children, specifically which condition associated with more stability and postural control ability with less postural muscle activity.
Fifteen right hemiplegic cerebral palsied children were recruited from the Outpatient Clinic of Faculty of Physical Therapy Cairo University and the National Institute of Neuromotor disorders and the children parents gave informed consent with procedure of the study. The protocol of this study approved by the ethical committees of the Faculty of physical therapy, Cairo University, Egypt
Their age range between 7 to 9 years of age chronologically, Spasticity ranged from 1to 1+ grades according to modified Ashworth scale, hemiplegia on right side of the body, Level Π gross motor function classification system, no surgical interference were performed within 2 years before participation or Botox intervention for 6 months prior to evaluation,, Able to understand procedures and follow directions. No history of any genetic or neurological disorders e.g. (epilepsy), no spinal deformities.
Kinetic analysis involves electromyograms (EMGS) with trigon wireless EMG system which consists of Delsys Surface EMG Sensors which are fixed parallel bar design, contoured shape, and convenient adhesive skin interfaces allow for consistent and hasslefree recordings, base station, delsys EMG software for acquisition and analysis of data.
Modified Paediatric Functional Reaching test which adapted for children in sitting position.
The children sat on rounded table without back support and adjustable foot support, they dressed in light clothes, an attractive bright coloured object was placed in front of the child in the midline at arm’s length at the level of his/her shoulder to encourage the child to perform unilateral forward flexion to the object with shoulder flexion 90 degrees. Children instructed to look directly forward and reach the object with affected right hand in normal speed and in a self-paced mode after a computerized go-tone. Participants moved and stopped their arms at a horizontal position for about 5sec before returning to the original position and instructed to maintain a fully extended position during arm movement, the children were tested under 3 conditions, they started in the standard sitting position on the table, which is characterized by horizontal orientation of the seat surface (condition 1), In two other condition a wedged platform was placed on the table. Participants performed three trials with interval 5 sec rest between each trial for the three conditions. The seat surface is manufactured and its dimensions is executed by taking average depth from back of the buttocks to back of the knee and the width by measuring widest area of hip for normal children from 7 to 9 years, The inclination is done with 15 degrees which induced a 15degrees forward (condition 2) or 15 degrees backward (condition 3). Delsys EMG sensors were placed over the following muscles on the affected side of the body of the hemiplegic cerebral palsied children, anterior deltoid (AD) which act as focal muscle of arm flexion, sternomastoid which act a, upper trapezius, thoracic extensors at level T10 bilateral, lumbar extensors at level l5 bilateral, rectus abdominals unilateral on the side of reaching. Thoracic extensors and lumbar extensors EMG signals are recorded bilaterally to record the activity of the muscles at both sides as previous studies indicated that higher EMG activity estimated from thoracic and lumbar extensors unilaterally at side of reaching in backward reclined position [22,23]. Leg muscle activity was not analysed, as previous studies as it is found that in typically developing sitting infants leg muscle activity is not related to postural control [24-26].
![Figure 1: Rt Hemiplegic cerebral palsy child in sitting position
during reaching on horizontal surface [A], forward inclined surface [B] backward inclined surface [C].](https://actascientific.com/ASPE/images/IJMCR/ASPE-07-0645-fig1.PNG)
Figure 1: Rt Hemiplegic cerebral palsy child in sitting position during reaching on horizontal surface [A], forward inclined surface [B] backward inclined surface [C].
EMG Root Mean Square (RMS) amplitude was measured to quantify the magnitude of postural muscle activity; (rt stern mastoid, rt upper trapezius, rt thoracic extensors, lt thoracic extensors, rt lumbar extensors and lt lumbar extensors) and it is expressed during burst activity of deltoid, the main flexor of shoulder, it is done by measuring the activity in window of burst activity of the deltoid after the onset of reaching.
The EMG data was normalized by measuring root mean square amplitude of submaximal voluntary contraction for each muscle divided by maximum voluntary contraction (MVC) of the same muscle divided by 100, the output is displayed as percentage of % MVC [27], can be used to easily establish a common background when comparing data. MVC normalization can be used to eliminate variance and allow data comparison between subjects to take place [28].
Analysis of variance (ANOVAS) used to determine the effect of the condition of the seat surface on amplitude of postural muscle activity and postural control ability in terms of forward reaching test during reaching in hemiplegic children, throughout the analyses, we considered differences with p values < 0.05 as statistically significant and with p values < 0.01 as highly statistically significant, Post hoc analysis used to determine loci of significance for this analysis.
This study shows an effect of seat surface inclination on postural muscle activity during reaching in sitting position, ANOVA reveals that there is significant difference between the three conditions in mean amplitude of rt trapezius, right, left thoracic extensors, left and right lumbar extensors muscle activity on the right affected side of the body as shown in table (1), post hoc analysis shows that there is significant difference between backward versus forward, backward versus horizontal and horizontal versus forward with p value <0.05 for Rt upper trapezius, Rt and left thoracic extensors, Rt and left lumbar extensors as shown in table (2) and this means that backward tilting position is associated with more muscular effort and less efficient while in forward inclined position.
In functional reaching test, the results shows there are significant difference between the three positions as shown in table (3), post hoc analysis shows significant difference between forward versus backward and forward versus horizontal with P value <0.05 as shown in table (4), this means that in sitting position during reaching, forward inclined position is associated with more forward reaching in other words better in postural control ability and stability.
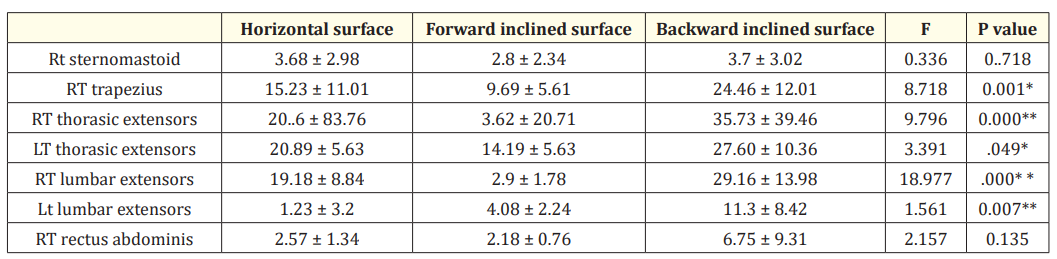
Table 1: Shows the mean amplitude values of the postural muscle activity during reaching in sitting on horizontal surface, forward inclined surface and backward inclined surface.*=statistically significant,**= highly statistically.
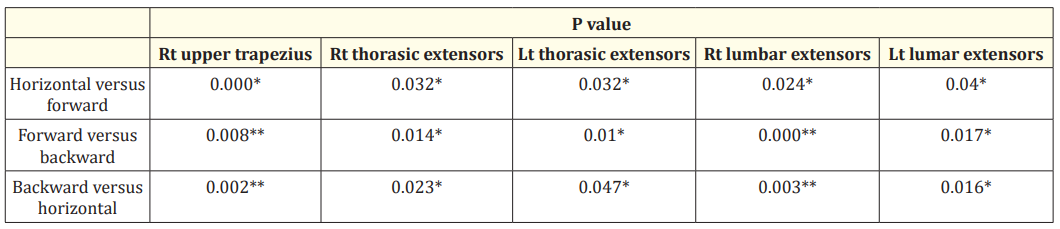
Table 2: Post hoc analysis Tests for comparing the activity of muscles of significant values among three positions during reaching in normal group. * statistical significant * * = highly statistically significant.

Table 3: Modified Paediatric Functional Reaching Test in the sitting on horizontal surface, on forward inclined surface and backward inclined surface.

Table 4: Post hoc analysis for Modified functional reaching test among three positions. *significant, ** highly significant, NS: nonsignificant.
![Figure 2: Example of EMG data of postural muscle activity for Rt hemiplegic child during reaching in sitting position on horizontal
surface [A], Forward inclined surface [B], backward inclined surface [c] The muscles are shown in the graph are rt anterior deltoid,
rt sternomastoid, rt upper trapezius, lt thorasic extensor, rt thoracic extensors, lt lumbar extensors, rt lumbar extensors, rt rectus
abdominals respectively.](https://actascientific.com/ASPE/images/IJMCR/ASPE-07-0645-fig2.PNG)
Figure 2: Example of EMG data of postural muscle activity for Rt hemiplegic child during reaching in sitting position on horizontal surface [A], Forward inclined surface [B], backward inclined surface [c] The muscles are shown in the graph are rt anterior deltoid, rt sternomastoid, rt upper trapezius, lt thorasic extensor, rt thoracic extensors, lt lumbar extensors, rt lumbar extensors, rt rectus abdominals respectively.
The present study was conducted to evaluate the effect of seat surface inclination on postural control during reaching in sitting position in hemiplegic cerebral palsied children, The children involved in the study ranged from 7 to 9years, at this age postural adjustment becomes comparable to adult pattern and stability limits of postural control approaches to adult levels at age of 7 years old [29,30].
Children of cerebral palsy often shows postural control dysfunction due to lack of motor control and weakness of muscles which should stabilise the trunk and pelvis [31], several studies showed that seat inclination have effect on pelvic tilt, postural muscle activity and balance [32], from this point of view our study use forward, backward inclined surface with 15 degree and horizontal surface to show their effect on postural activity during reaching.
Forward inclination of the seat provides a more upright and stable posture and controls the abnormal kyphosis [33] With this kind of sitting position, the centre of gravity shifts forward, lumbar extension time increases, the backward rotation of pelvis is prevented, and tightness of hamstring and back extensor muscles activity decreased and this agrees with the present study in which the normal postural alignment created by forward inclined seat surface does not require higher activity from back extensors and this was shown from the post hoc statistical analysis in which activity of rt upper trapezius, rt, lt thoracic extensors and rt, lt lumbar on the side of reaching shows significant difference in forward versus backward, forward versus horizontal with forward inclined position with lesser activity.
McClenaghan., et al. 1992 [36] studied 20 children with CP with an age range of 4–10 years, and examined their upper extremity functionality by placing them in seats with varying inclinations while they were performing their daily activities. They reported no significant difference among groups (straight, tilted forward, tilted backward) regarding upper extremity functionality and this disagree with our study as modified paediatric reaching test which measure the postural control ability and upper extremity reaching shows significant difference between the three position with forward inclined position higher forward reaching from post hoc analysis.
The present study shows significant difference in activity of rt trapezius, Rt, lt thoracic and Rt, lt lumbar extensors at the side of reaching between the three position in which backward inclined position shows the higher activity from post hoc analysis, this could be explained that increase in back muscle activity in backward reclined position used to realign of the kyphotic posture obtained from posterior tilting of pelvis.
In this study there is significant difference in modified paediatric functional reaching test in the three positions with forward inclined position is associated with more forward reaching in comparison with backward and forward inclined positions from post hoc analysis, this is could be explained by the 15 degree inclination provide slight anterior pelvic tilting which provide slight range of forward movement within limits of stability that compensate form insufficient range of reaching due to less force production, coordinated movement limitations, and reduced efficiency of hand transportation towards targets in children with cerebral palsy children [37,38].
Hadder-algra., et al. 2007 [39] states that in the children with unilateral spastic CP, forward tilting improved postural efficiency and improve quality of reaching) and Rong., et al. (2009) [40] states that anterior-inclined position improve postural stability and reaching efficacy, this agrees with our study as there is a significance increase in modified reaching test in forward inclined position which reflect the stability limits, postural control ability and the amount of reaching.
Post hoc analysis shows significant difference between forward and backward positions, this may be due to in backward position there is a great tendency to sit on the sacrum [41] and the child exert much effort in leaning forward due to excess activity of the Rt trapezius, Rt thoracic, Rt lumbar extensors muscles to maintain alignment of posture and this limits the ability of reaching and decrease the limits of stability.
The present study shows that the forward inclined seat surface is more efficient than backward inclined and horizontal seat surface as forward inclined position associated with less postural muscle activity and more postural control ability in terms of modified paediatric reaching test.
Copyright: © 2024 Enas Hamdy Elnady., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.