Bilel Zakaria Samari*, Samia Krioudj and Zineddine Soualili
Pediatric Surgery Department, Laboratory of Applied Pediatric Surgery, Mother and Child Hospital, FERHAT Abbas University, Setif, Algeria
*Corresponding Author: Bilel Zakaria Samari, Pediatric Surgery Department, Laboratory of Applied Pediatric Surgery, Mother and Child Hospital, FERHAT Abbas University, Setif, Algeria.
Received: February 13, 2023; Published: May 25, 2023
Citation: Bilel Zakaria Samari., et al. “Splenic Torsion in Childhood: A Case Report”. Acta Scientific Paediatrics 6.6 (2023): 21-22.
Splenic hypermobility is due to laxity or absence of supporting spleen ligaments. Its clinical presentation is variable and it may lead to an acute abdomen due to a pedicle torsion. We describe here a pediatric case of an acute splenic torsion secondary to a wandering spleen happened to a 2 years old girl who presented with abdominal pain and vomiting. Ultrasonography and CT scan showed an ectopic spleen with hypo-enhancement and the diagnosis of splenic torsion was highly suspected. The girl underwent a laparotomy that confirmed the diagnosis and a detortion was performed with a splenopexy.
Keywords: Wandering Spleen; Torsion; Splenopexy
Splenic torsion is a rare emergency in childhood, and it seems to occur in another rare clinical entity; the wandering spleen. Which can be less evident to diagnose due to its poor symptomatology, therefore most of children presenting an anomaly of the supporting ligaments remains asymptomatic. However an acute abdomen can be the expression of a splenic torsion.
We report the case of a 2 years old girl presented with a fivedays history of abdominal pain, alimentary emesis. The pain was initially thought to be due to constipation. On physical exam, her abdomen was diffusely tender with the palpation of a mass in the right flank. Laboratory analysis demonstrated: WBC 11000/μL, hemoglobin 8 g/dl, platelets 383 103/μL, and a normal urinalysis. US showed an ectopic splenomegaly. A CT scan was performed, and showed an abnormal medialization of the spleen, likely related to wandering spleen.
Additionally, there was abnormal splenic hypo-enhancement, edema, and surrounding inflammation with swirling of the splenic vascular pedicle (Figure 1).
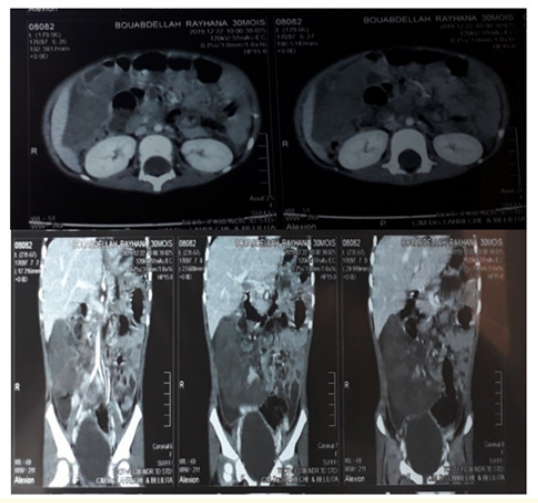
Figure 1: CT scan showing a swelling ectopic spleen within the right flank.
A splenic torsion is highly suspected and the patient underwent an urgent laparotomy. Which showed a torsed wandering spleen in the right flank with three spires on its vascular pedicle.it was untwisted with total recovery of blood flow (Figure 2). A splenopexy was performed and pathologic inspection confirmed hemorrhagic congestion without splenic infarction.
The patient recovered uneventfully and was discharged with anti-aggregation therapy for a thrombocytosis at 900.10^9/L.Post-operative Doppler US demonstrate a normal blood flow.
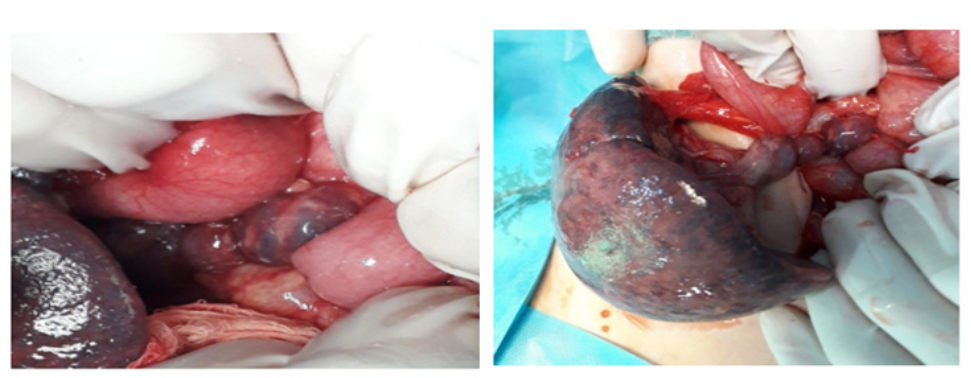
Figure 2: Intraoperative photo showing the torsion of vascular pedicle.
Wandering spleen is an exceedingly rare condition, accounting for less than 0.2% of all splenectomies [2]. In the pediatric population it is due to a congenital abnormality of the splenic ligaments. The spleen develops from an aggregation of mesenchymal cells in the dorsal mesentery of the stomach. The splenorenal ligament results from the fusion of the left surface of the mesogastrium and the peritoneum over the left kidney. The splenic vessels course through this structure [3]. A congenital failure of normal splenic ligament fusion during embryogenesis leads to increased laxity of the gastrosplenic and splenorenal ligaments and allows for hypermobility of the spleen [1,4]. This hypermobility leads to complications as : splenic torsion, splenic infarction, splenic vein thrombosis, small bowel obstruction, pancreatitis, and gastric outlet obstruction. Splenic torsion, infarction and venous thrombosis are attributable to the spleen twisting on its vascular pedicle and ultimately disrupting blood flow to and from the spleen. Small bowel obstruction, pancreatitis and gastric outlet obstruction are likely due to mass effect from an enlarged spleen. In adult patients, this can be an acquired condition, most commonly seen postpartum secondary to ligament laxity following pregnancy related hormonal changes [5]. Additionally, wandering spleen can be challenging to treat since patients often present after experiencing a complication.
A triad of physical exam findings associated with wandering spleen are palpable, hard, and ovoid abdominal mass; painless movement of the mass toward the left upper quadrant but limited in all other directions, and resonance to percussion in the left upper quadrant [6]. These findings; however, are not consistently seen in patients with wandering spleen, so diagnosis requires more than physical exam alone. CT imaging is commonly used to further characterize a potential mass found on exam or locate the wandering spleen in the abdomen. Common CT findings includes: an empty splenic fossa, an ectopic spleen and a whirl sign which is a sign of splenic torsion [2]. Doppler ultrasonography is the most commonly used imaging [7] since it can characterize the mass and assess blood flow in cases of splenic torsion. The most specific US finding for wandering spleen is low position of the spleen [8].
Management of wandering spleen is surgical, with the treatment options being splenectomy and splenopexy. Traditionally, splenectomy was the treatment of choice to prevent future complications, but splenopexy has replaced splenectomy in cases without splenic infarction [9] for preservation of splenic immune function. Splenopexy can be done in several ways. Traditionally this was an open procedure, where the splenic capsule was sutured to the undersurface of the diaphragm [10]. This technique; however, was prone to capsular tear and bleeding, so newer techniques were developed. Splenic preservation and fixation is now most commonly performed by laparoscopy with construction of an omental or retroperitoneal pocket or with the use of mesh to fix the spleen in the left upper quadrant of the abdomen [10]. It should be noted that when the spleen is unable to be preserved, the individual is at increased risk for infection by encapsulated bacteria and the Advisory Committee on Immunization Practices (ACIP) recommends a more intensive vaccination schedule [11]. Additionally, children should receive at least 1-2 years of antibiotic prophylaxis postsplenectomy and some experts recommend life-long prophylaxis [12].
We report a case of pediatric splenic torsion secondary to congenital absence of normal ligamentous splenic attachments with an uneventful recovery after the untwist and the splenopexy. While rare, this diagnosis must be considered as a cause of abdominal pain in patients who have imaging that demonstrates an abnormal splenic attachments.
Copyright: © 2023 Bilel Zakaria Samari., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.