Márcio Luís Duarte1,2, Thaís Amanda Frank de Almeida Alves3, Marco Antonio Alves Braun3, Lucas Ribeiro dos Santos2,3 and Élcio Roberto Duarte4*
1WEBIMAGEM TELERRADIOLOGIA, Santos, São Paulo, Brazil
2Master Degree in Evidence-Based Health at UNIFESP, São Paulo, São Paulo, Brazil
3Faculdade de Ciências Médicas de Santos, Santos, São Paulo, Brazil
4Irmandade da Santa Casa de Misericórdia de Santos, Santos, São Paulo, Brazil
*Corresponding Author: Élcio Roberto Duarte, Irmandade da Santa Casa de Misericórdia de Santos, Av. Dr. Cláudio Luiz da Costa, Jabaquara, Santos - SP, Brazil.
Received: August 13, 2021; Published: September 25, 2021
Citation: Élcio Roberto Duarte., et al. “Edwards Syndrome - A Rare Trisomy”. Acta Scientific Paediatrics 4.10 (2021): 83-86.
Chromosome 18 trisomy is a chromosomal disorder due to the presence of an extra 18 chromosome, mosaic trisomy, or partial 18q trisomy. The prevalence of live births is estimated at 1: 6000-1: 8000. The ultrasound is vital for the suspicion of chromosome 18 trisomy, especially when the changes refer to the clenched fists with overlapping fingers. However, the diagnosis of certainty is still the karyotype because, in some cases, changes may not be seen on ultrasound examination. We report a case of a 39 years-old woman perform an obstetric ultrasound at about 22 weeks showed the “lemon head” sign and constantly clenched fists of the fetus during the exam, suspecting Edwards Syndrome. After birth, at physical examination, the fists clenched with the fingers of both hands. The karyotype confirmed the trisomy of chromosome 18.
Keywords: Fetus; Infant; Newborn; Trisomy 18 Syndrome; Ultrasonography; Prenatal Care
Chromosome 18 trisomy, also known as Edwards syndrome, is a chromosomal disorder due to the presence of an extra 18 chromosome, mosaic trisomy, or partial 18q trisomy [1-3]. The prevalence for live births is estimated at 1: 6000-1: 8000 [2]. It is the second most common trisomy, behind only the trisomy of chromosome 21 - Down syndrome [1,2].
This syndrome is associate with a high frequency of fetal loss and pregnancy termination after prenatal diagnosis [2]. The complexity and the severity of the clinical presentation with multiple congenital anomaly syndromes requires multiple pediatric and specialist evaluations once 50% of babies with trisomy 18 live more than a week, with an average survival of two weeks and about 5 - 10% of children beyond the first year, presenting rare long-term survival [2-4].
The recognizable pattern of the syndrome consists of major and minor anomalies (Table 1) [2]. The ultrasound is vital for the suspicion during prenatal examinations especially when the changes refer to the clenched fists with overlapping fingers [9]. However, the diagnosis of certainty is the karyotype [2].
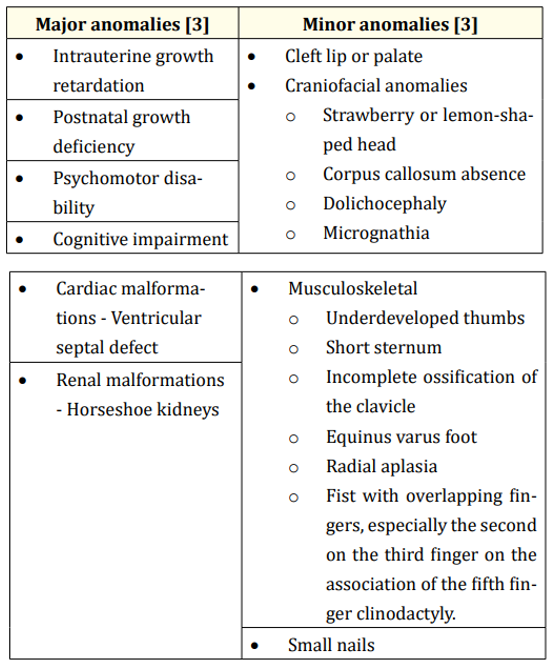
Table 1: Summary of the most common major and minor anomalies.
A 39 years-old woman presented gestational hypertension being controlled with methyldopa. She performed seven prenatal consultations, with no complications. HIV serologies, IgM toxoplasmosis, Hepatitis C, and rubella IgM negative. Toxoplasmosis IgG, anti-Hbs, and rubella IgG reagents.
During pregnancy, an ultrasound at about 22 weeks showed the “lemon head” sign (Figure 1) and constantly clenched fists during the exam (Figure 2). With 29 weeks of pregnancy according to the date of the last menstruation, the ultrasound demonstrated a restriction of intrauterine growth, as it presented, according to the exam measures, about 26 weeks and five days. Four weeks later, in addition to the growth restriction, weight below the 10th percentile for gestational age was added. After four more weeks, the weight was below the 5th percentile for gestational age.

Figure 1: Ultrasonography showing the fetus with the “lemon head” sign (white arrow).

Figure 2: Ultrasonography showing the fetus with clenched fists with the fingers of both hands folded. R HAND: Right hand. L HAND: Left hand.
The newborn was born by cesarean delivery having 40 weeks and 05 days for the last menstrual period (LMP). He was transferred to the ICU due to acute respiratory failure, where he was intubated. On physical examination, the patient is anicteric, afebrile, discolored and pale, hypoactive/hyporeactive, and spastic. Cardiac auscultation was normal - 116 heart rate. Pulmonary auscultation detected a 2+/4+ systolic murmur, with snoring and crackling rales, with a respiratory rate of 38 breaths/min, saturating about 93%. Blood pressure of 100 x 70 mmHg. Flat and normotensive fontanelle. Globose abdomen, with a palpable liver 3 cm from the right costal margin. It was also noted some peculiarities such as facial hirsutism, micrognathia, triangular head, reducible bilateral inguinal hernia, reducible umbilical hernia, and the fists clenched with the fingers of both hands (Figure 3). The karyotype confirmed the trisomy of chromosome 18.

Figure 3: Physical examination showing the newborn with clenched fists with the fingers of both hands folded.
Chromosome 18 trisomy, also known as Edwards syndrome initially described in 1960, is a chromosomal disorder due to the presence of an extra 18 chromosome, mosaic trisomy, or partial 18q trisomy [1-3]. Changes can be caused by abnormal expression of genes important for development on chromosome 18 [4]. Nondisjunction is the leading phenomenon, during the second meiotic division of maternal oogenesis [2]. Translocations and mosaicism are less frequent, corresponding to milder manifestations and being observed in only 10% of cases [3].
The prevalence for live births is estimated at 1:6000 - 1:8000, but the gestational prevalence is higher (1:2500 - 1:2600), due to the high frequency of fetal loss and termination of pregnancy after prenatal diagnosis [2]. Its prevalence rises with increasing maternal age and presents a risk of recurrence for a family with a child with a complete trisomy of about 1% [2].
Although infant mortality is well known to be inevitably lethal, about 50% of babies with trisomy 18 live more than a week, with an average survival of two weeks and about 5 - 10% of children beyond the first year, presenting rare long-term survival [3,4]. All long-term survivors have severe mental retardation and spasticity [5]. Male fetuses appear to be more likely to miscarriage than female fetuses, even though females are the most commonly affected by the syndrome, in a proportion of 3:1 over boys [1].
These anomalies involve the urogenital tract, cardiovascular, craniofacial, and central nervous system [2,3]. The recognizable pattern of the syndrome consists of major and minor anomalies, with major malformations being the most common cardiac and renal anomalies (Table 1) [2].
Anomalies in the hands are highly suggestive of Edwards Syndrome during prenatal examinations [6]. The auricular bones of fetuses with Edwards Syndrome, according to Chrobok., et al. sometimes present abnormalities of the outer or middle ear and delayed ear development internal - no ossification of the optical capsule and the organ of Corti [7].
Despite the classic description, anomalies of the limbs can be very variable [8]. Some patients may present unusual changes, and these findings are extremely important for the clinical suspicion and early identification of these patients [8]. The early-onset intrauterine growth retardation, dysmorphism of the facial skeleton, congenital malformation such as protruding occiput, equine foot, radial aplasia, cleft lip or palate, cryptorchidism, malformations of the extremities, especially of the palms and feet found in the newborns suggest the diagnosis of Edwards Syndrome [2]. Bone changes occur with the eleven pairs of ribs that are present and are classically hypoplastic and thin with the short sternum makes the deformity look like a shield in the chest and with the iliac angle, which, if acute, is a diagnosis of the syndrome [7].
Ultrasonography shows practically 100% sensitivity for visualizing structural anomalies, such as increased nuchal thickness, delayed intrauterine growth, choroid plexus cyst, cerebellar hypoplasia, overlapping fingers, diaphragmatic hernia and congenital heart defects - interventricular and/or interatrial communication and a single umbilical artery in 80% of cases [2,9]. Omphalocele also speaks in favor of chromosomal disorders, with Edwards Syndrome being the most common trisomy, followed by trisomy 13 [10]. Currently, most cases of chromosome 18 trisomy are suspected in prenatal care, based on screening for maternal age, screening of the marker in the maternal serum, or the detection of ultrasound abnormalities [2,9].
Edwards Syndrome has several differential diagnoses, such as trisomy of chromosome 13 or chromosome 9, Cockayne syndrome, Werdnig-Hoffman’s disease, and Pena-Shokeir syndrome [5,9]. Nevertheless the clenched hand - index finger overlaps a clenched fist formed by the other digits - constant during the ultrasound is powerfully indicative of trisomy 18 [9]. It needs to be differentiated from a fixed position seen in akinesia-hypokinesia syndromes and from a momentarily closed but normal fist [9].
The leading causes of death include central apnea, heart failure due to cardiac malformations, respiratory failure due to hypoventilation, aspiration or obstruction of the upper airways, and probably the combination of these and other factors - including decisions regarding intensive care [2]. The complexity and severity of clinical presentation at birth and high neonatal mortality and perinatal and neonatal management of babies with trisomy 18 are particularly challenging and may require multiple pediatric and expert assessments, including consistently occurring feeding problems [2].
In cases of trisomy of the 18 chromosome, there´s no indication to perform a cytogenetic evaluation of the parents, because this abnormality is due to a phenomenon of nondisjunction during gametogenesis [1].
The authors declare that there is no conflict of interest regarding the publication of this paper.
Copyright: © 2021 Élcio Roberto Duarte., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.