Sonali S1 and Edwin Dias2*
1Senior Research Scholar, Srinivas University, India
2Head of Pediatric Department, SIMS, Mangalore, India
*Corresponding Author: Edwin Dias, Head of Pediatric Department, SIMS, Mangalore, India.
Received: July 22, 2021; Published: September 24, 2021
Citation: Sonali S and Edwin Dias. “Effectiveness of Matrix Rhythm Therapy with Traditional Physiotherapy for Child with Spastic Diplegic Cerebral Palsy from 13 Months to 7 Years Age: A Case Report”. Acta Scientific Paediatrics 4.10 (2021): 78-82.
This case study shows the effectiveness of matrix Rhythm therapy for 13 month old girl with Cerebral palsy. The aim was to find out the effectiveness of matrix rhythm Therapy when combined with traditional physiotherapy to improve gross motor function.. Before starting physiotherapy treatment the girl had lots of impairments on gross motor function and GMFCS level was 3. On Denver developmental scale evaluation she was 8 month behind in two subgroups of gross motor and fine motor. MACS level was 3. CFCS level 1. The child still continues Physiotherapy session at the age of 7 years once a month. After receiving intensive Physiotherapy she improved in gross motor function specially sitting standing walking stair climbing and jumping. As well improvement was seen in balance and posture. The modified Ashworth scale, goniometry evaluation, GMFM-88, MACS, CFCS, Pediatric Berg balance scale were used as outcome measure. There was drastic improvement seen in GMFM SCORE after Matrix Rhythm therapy combined with traditional physiotherapy for this type of cerebral palsy.
Keywords: Matrix Rhythm Therapy; Cerebral Palsy; Gross Motor; Fine Motor
Cerebral palsy is one of the most challenging motor orders in children. Cerebral palsy describes a group of permanent disorders of development, of movement and posture causing activity limitation that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of cerebral palsy are often accompanied by disturbances of sensation, perception, cognition, communication and behaviour, by epilepsy and by secondary musculoskeletal problems. Spastic diplegia Cerebral palsy is amongst the most common types.
It is developed by DR. U.G. Randoll in Earlangen’s university Germany. This therapy is based on the research in cell biology. Our cells are pulsating in frequencies of 8-12 hertz in normal healthy condition. During unhealthy situation these movements are slowed down. Marhythe The provides populations in same frequency to synchronize and reset the disturbed cell rhythm that helps to reestablish extra cellular logistics that is removal of waste products and improve microcirculation of with oxygenated blood. It relaxes soft tissues.
Child was born on 7 August 2014. First Physiotherapy evaluation was done on 5th September 2015. History revealed that child was born full term through LSCS as healthy child. Child had cried loudly and was not admitted to NICU. She didn’t had any respiratory distress or any other high risk factors. Mother was considered at risk of developing hypertension. MRI revealed changes in bilateral cerebral hemisphere with volume loss and mild ex-vacuo prominence of bilateral cerebral white matter. There is prominence of bilateral cerebral sulcus space. Thinning of Corpus callosum was seen. Small focus of gliosis was found in left cerebellar white matter. The evidence revealed history of hypoxic ischemic encephalopathy.
Child was assessed thoroughly. Assessment was done at consecutive ages still 7 years. Treatment was given one hour daily 5 days a week from 13 months to 2 years. Bi weekly sessions were given from 2 years age still 3 years. Follow up was done every month from three years to seven years of age.
Functional goals- Independent dressing, eating, bathing, grooming transfers.
Multisystem is affected which includes tone, alignment, posture, balance, coordination. In child with cerebral palsy independence in functional skills depends upon some or all developmental areas as motor, sensory, cognitive, communication behaviour. The child also needs to recognise the social needs. GMFCS level was achieved to Level 1 at the age of two and half years. It was level 5 at the age of 13 months. GMFM score improved from 0 to 209 (2 years) and was maximum after 5years. Pediatric Balance score improved from 0 at the age of 13month to 17 at the age of 2 years. The maximum score was achieved after 6 years. Table 4 clearly depicts changes in GMFM and MAS score proving maximum improvement was seen between 13months and 2 years. The overall effect was 1210 times at the age of 7 years in GMFM score. The MAS score showed improvement by 560 times at the age of 7 years [1-7].
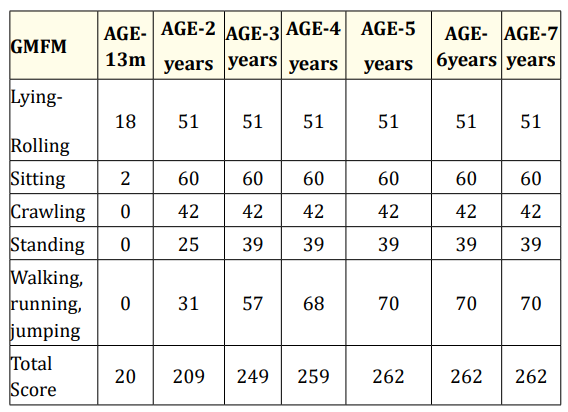
Table 1: Gross motor function measure scores at various age of child.
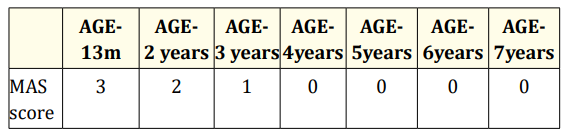
Table 2: Modified ash worth scale at various ages of child.
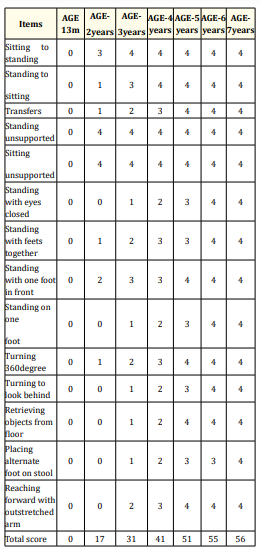
Table 3: Pediatric berg balance score at various ages of child.
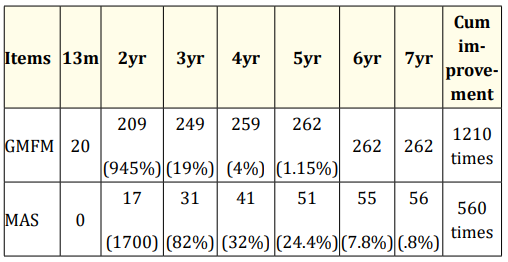
Table 4: Improvement analysis in Gmfm and mas score across the age till 7 years.
Matrix rhythm therapy effectively optimised the muscle tone of cerebral palsed child in less than expected time duration. The combined therapeutic approach kept child and family motivated to continue efforts till goals were achieved completely. The child’s overall performance is appreciated as above average in school, home and community settings.
Nil.
No conflict of interest.
Copyright: © 2021 Sonali S and Edwin Dias. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.