Fatima Bello Jiya1*, Tahir Yusuf1, Nma Muhammed Jiya1, Mohammed Yahaya2, Paul Kehinde Ibitoye1, Asma’u Adamu1, Khadijat Omeneke Isezuo1 and Maryam Amodu-Sanni1
1Department of Paediatrics, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria
2Department of Medical Microbiology and Parasitology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria
*Corresponding Author: Fatima Bello Jiya, Department of Paediatrics, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria.
Received: December 01, 2020; Published: February 22, 2021
Citation: Fatima Bello Jiya., et al. “An Assessment of Illness Perception of Caregivers of Children Attending Antiretroviral Therapy Clinic of a Tertiary Health Facility in North-west Nigeria”. Acta Scientific Paediatrics 4.3 (2021): 70-75.
Background: The perception of illness among individuals is a phenomenon that has been described as processes by which Individuals diagnosed with an illness, health threat, or an injury are said to develop an organized pattern of beliefs about their condition. These beliefs are developed not only in persons suffering from ill health but also among close companions.
Objective: To determine the perception of caregivers of children infected with Human Immune deficiency Virus (HIV) attending antiretroviral therapy (ART) Clinic of Usmanu Danfodiyo University Teaching Hospital (UDUTH) Sokoto.
Methods: A cross-sectional study involving consenting primary caregivers of children aged 15 years and below diagnosed with HIV, attending ART clinic of UDUTH Sokoto. They were recruited from July to December 2018. Data collected were demographics, information regarding illness perception was adapted from the brief illness perception questionnaire and data was analyzed using SPSS version 23.
Results: Ninety four consenting caregivers participated in the study. Mean age was 36.8± 8.0 with M:F of 1: 5.7. Mean age of the children was 9.1 ± 3.9, with M:F of 1.1:1.Majority 58 (6 1.7%) were of low social class. The cause of HIV was believed to be germs in 66(70.2%), with a chronic timeline by 54(57.4%) of caregivers. Sixty four (68.1%) of them perceived no major consequences on the child’s future. Majority 75(79.8%) had no control over child’s illness. Almost all caregivers 92(97.9%) believed treatment will control the infection. Fear 36(38.3%) and distress 17(18.1%) were the commonest emotions among caregivers and 65(69.1%) believed they understood child’s illness very much.
Conclusion: Caregivers had good cause of illness comprehensibility. However, the perceived consequences, emotional, and personal control were low.
Keywords: Illness Perception; Caregiver; Human Immunodeficiency Virus Infection; Children; Sokoto
The perception of illness among individuals is a phenomenon that has been defined using self-regulatory models that are said to describe processes by which people react to a perceived health threat [1]. Individuals diagnosed with an illness, health threat, or who suffer an injury are said to develop an organized pattern of beliefs about their condition and the cognitive and emotional representations of the illness, or illness perceptions is said to determine the individual's coping behavior [1,2]. Psychological representation of ill health may depend on the age, cognitive development, disease condition and environmental factors that could influence people’s beliefs concerning their health conditions. These beliefs can be developed not only in persons suffering from ill health but also among close companions [2]. In the case of children suffering from disease conditions, the caregiver is also expected to develop coping strategies to adapt to the child’s needs especially in the setting of chronic illnesses. Generally, caregivers from within the family are said to bear important and multidimensional responsibilities over time in order to manage a chronic disease and usually suffer various financial, family, social, mental and psychological problems [3,4]. Negative illness perceptions are associated with poorer recovery and increased healthcare use independent of objective measures of illness severity [2]. Caregivers of children with certain disease conditions for which cure is yet to be established such as human immune deficiency virus (HIV) infection are at risk of psychological disturbances and might find it difficult to express selves out of fear of being judged unfairly. Additionally, such diseases in which stigmatization and discrimination of affected people still exists further compounds the perception of caregivers and patients of sufficient age with resultant emotional imbalance [5-7]. It might also be perceived as culturally unacceptable in some societies to discuss certain personal or private issues concerning self or family with non-family members because such issues might have sociocultural implications. Psychological instability of the caregiver could be detrimental to the care offered to affected children and can interfere with their growth and development, in the face of an already existing medical condition. There had been reports of illness perception assessment among adults and caregivers of children in the developed countries using the illness perception questionnaire and its various modifications with positive results [8-12]. The awareness of patients’ as well as caregivers perception of illness is likely to improve communication, reduce disability and improve treatment outcome [12]. There is no known study on perception of child’s illness by caregivers of children infected with HIV in the study location, despite owning and offering functional Paediatric antiretroviral therapy (ART) services to HIV infected and exposed children. We sought to determine the perception of caregivers of children infected with HIV attending antiretroviral therapy (ART) Clinic of Usmanu Danfodiyo University Teaching Hospital (UDUTH) Sokoto, North – Western Nigeria, with the aim of detecting positive and negative perceptions regarding HIV infection and its effects, improving communication between attending doctors and caregivers, and using the information generated to further strengthen the already existing counselling services within the health facility.
The study was conducted at the Paediatric ART clinic of UDUTH Sokoto, a tertiary health facility located in Sokoto, the Capital of Sokoto State, North –Western Nigeria. The hospital serves as a referral center for people of Sokoto, Kebbi, Zamfara, Niger and Katsina States of Nigeria. The Paediatric ART Clinic of UDUTH offers free medical services using available resources and it is overseen by specialists in the field of Paediatrics with an average of twenty HIV infected and exposed children being attended to on weekly basis.
The study was a cross-sectional survey that involved caregivers of children aged 15 years and below infected with HIV, attending the Paediatric ART clinic of UDUTH Sokoto. They were consecutively recruited during ART clinic visits over a 6 month period from July 2018 to December 2018. Ethical approval for the study was obtained from the Health Research and Ethics Committee of UDUTH. The inclusion criteria for participants were physical identification as primary caregiver of HIV infected children aged 15 years and below and informed written consent. Caregivers of HIV infected children with acute illness or with other co morbidities such as sickle cell disease, congenital abnormalities, malignancy, critically ill children with Acquired Immune Deficiency Syndrome (AIDS) defining illnesses requiring frequent hospital admission and children not accompanied by primary caregivers were excluded. A primary caregiver was defined as an adult 18 years and above, living in the same household as the child in question, who was ordinarily responsible for supervising the care of the child in the home and for bringing the child to the hospital for his/her regular clinic visits.
Subjects that satisfied the inclusion and exclusion criteria were recruited into the study. Designed pretested questionnaires were used to document information obtained from the caregivers which included; demographics such as age, gender, address, ethnicity and socio-economic status of caregivers using Oyedeji classification [13]. Questions regarding illness perception were adapted from the brief illness perception questionnaire, a reliable and validated instrument that can be applied to rapidly assess the cognitive and emotional representations of illness using 9 items. The items include the causal question, 5 items assessing the cognitive illness representation; consequences, personal control, treatment control, identity and timeline, two items assessing emotional representation; concern and emotions, while 1 item assesses illness comprehensibility [2]. Privacy was ensured by interviewing a caregiver in a separate room provided for the purpose of the study and away from other caregivers and patients, for an average of 20-30 minutes. To be sure they understood the questions, there were recaps of some of the questions as well as the responses gotten from the caregivers. Data obtained was treated with utmost confidentiality.
Data was analyzed using statistical package for social sciences (SPSS) version 23.0. Data entered was carefully checked to eliminate multiple or wrong entries, missing values, and outliers. The age distribution of the caregivers and subjects were analyzed and expressed as mean and standard deviation while gender was expressed as percentages and ratio. Frequency distribution tables were used to illustrate results. Comparison between groups were made using Chi square or Fischer’s exact test where applicable. The level of statistical significance was set at 5%, which is p-value < 0.05.
Ninety four consenting caregivers participated in the study. The caregivers age ranged from 21 years to 58 years, mean age was 36.8 ± 8.0. The caregivers were made up of 80(85.1%) females and 14 (14.9%) males with M: F of 1: 5.7. The children’s age range was 1 to 15 years, with mean (S.D) of 9.1 ± 3.9 comprising of 50 (53.2%) males and 44 (46.8%) females with M: F of 1.1:1. Fifty eight (61.7%), 20(21.3%), and 16(17.0%) were of low, middle and high social class respectively. (Table 1). Fifty four (67.5%) of the females were unemployed and their social status was significantly lower (p = 0.007) than those of the male caregivers.
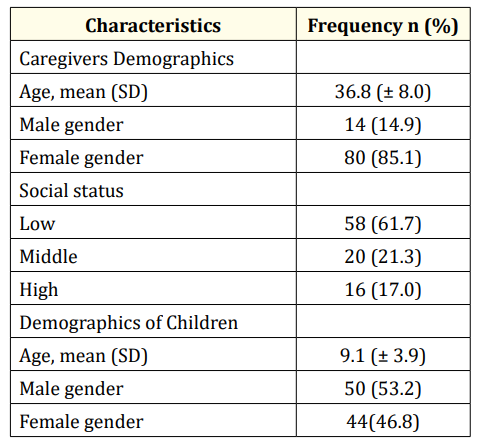
Table 1: Demographic Characteristics of Caregivers and Patients.
Fifty seven (60.6%) of the caregivers had been aware of the HIV status of the patients for at least 5 years before the survey. The cause of HIV infection was believed to be germs in 66(70.2%), hereditary in 9(9.6%) and spiritual in 5(5.3%) of caregivers (Table 2). Human immunodeficiency virus was believed to be an acute illness by 11(11.7%), chronic by 54(57.4%) and permanent by 29(30.9%) of the caregivers. Of the 94 caregivers, 44(46.8%) did not perceive HIV as a serious condition. Thirty seven (39.4%) of the caregivers believed the infection had no effect on the child’s life while 33(35.1%) felt there was little effect on the child. Sixty four (68.1%) caregivers perceived no major consequences on the child’s future (Table 3).

Table 2: Caregivers’ Cognitive Perception of Illness.

Table 3: Emotions, Personal Control and illness Comprehensibility of Caregivers.
Majority 75(79.8%) of the caregivers perceived no control over child’s illness. Almost all caregivers 92(97.9%) believed treatment will control the infection. Fear 36(38.3%) and distress 17(18.1%) were the commonest emotions among caregivers. Seventy six (80.9%) caregivers were concerned about child’s illness and 65(69.1%) understood child’s illness very much. Comparing the duration of awareness of child’s HIV status and perceived care givers emotions as well as illness comprehensibility, there was no significant difference (p = 0.90) between caregivers in terms of the duration of awareness of child’s diagnosis being either less than 5 years or 5 years or more.
There was no statistically significant difference in the perception of causal factor between the male and female caregivers (p = 0.97). There was also no difference in the caregivers perception of the timeline (p = 0.51) of HIV infection. Male caregivers had significantly higher (p = 0.04) perception of the consequences of HIV on the children than female caregivers. The difference in the perception of control over child’s illness was not significant between male and female caregivers (p = 0.80) (Table 4). Comparing the duration of awareness of child’s HIV status and perceived caregivers emotions, revealed no significant difference (p = 0.90). However, illness comprehensibility increased significantly (p = 0.04) with caregivers duration of awareness of child’s illness above 5 years.
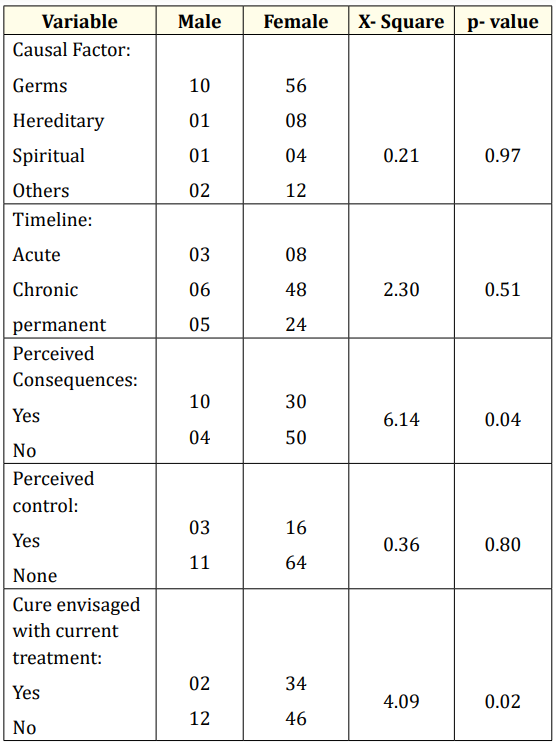
Table 4: Relationship between Caregiver’s Gender and Illness perception.
The caregivers in this study were predominantly females, which is in agreement with other studies of caregivers of children with chronic diseases. Females have been reported to assume the caregiving role more readily than the males. It has also been observed that mothers accept higher responsibilities than other members of the family and bear higher caregiving burden than fathers [14-18]. In this study, the duration of caregivers awareness of child’s HIV status seem not to have had impact on their emotional representation, suggesting that time had little or no effect on the development of coping strategies or otherwise of the caregivers.
The low socio economic and employment status of caregivers in this study is also in consonance with the studies in Ghana, Iran, and Brazil where most of the subjects had low Educational status and were unemployed or self-employed [16-18]. The finding in this study is not surprising as majority of the caregivers constitute females who in this region of the country are more at a disadvantage in terms of educational attainment and employment opportunities. Majority of the caregivers in this study had good perception of causal factor being a microorganism and timeline for HIV infection being chronic for the time being. This finding is contrary to that of Elijah et al in Ghana were most of the caregivers had inaccurate knowledge of HIV transmission [14]. Although most of the caregivers in our study had low educational status, the reason for the good cause and course of illness perception could be related to the health educational sessions that the caregivers are often exposed to at each clinic visit, in addition to other means of knowledge acquisition and information dissemination such as the media stations. The aforementioned reasons might also explain the increasing caregiver comprehensibility of child’s status in those with diagnosis of five years or more in this study.
The implication of HIV infection on the patient’s life and future were however, not well understood by most of the caregivers. It could be related to the possibility of information being provided to caregivers during counselling sessions as not likely addressing indepth, the consequences of the child’s illness. Although counselling usually has the effect of restoring hope in individuals affected by illness in a peculiar way, exaggerations on the part of health care providers might lead to unrealistic expectations by the caregivers. It is likely to be detrimental to the patients as the caregivers might out of false hopes fail to accord the illness the necessary or adequate attention it deserves. By extension, at an age when the patients have developed a cognitive level enough to understand the implications, the caregivers might not have been furnished with the ability to assist them transit through the critical stage of accepting the realities of their illness.
Caring for sick children especially in the setting of a chronic illness like HIV is said to be capable of depleting the energy of caregivers and exposes them to physical and emotional problems [14,16]. Fear, distress and blame were the major emotional representations of caregivers in this study. Their awareness of the timeline of HIV infection could explain the emotions. Being a chronic illness, the patients and their caregivers are likely to undergo long term rigors of health care visits and health conditions that might necessitate in-patient care with increasing caregiver burden. Their low social status might have also contributed to these negative emotions, considering the fact that the healthcare needs of these children usually require additional funds and time away from income generating ventures that would’ve supported the caregivers’ ability to carter for them. The aforementioned possibilities could also explain the perceived lack of personal control by the caregivers over child’s illness. Lack of family and other social support might also be attributed to these emotions because in a setting where stigmatization still plays a role in the lives of HIV infected individuals, it becomes difficult or almost impossible to confide in, and seek psychological and financial support from relatives and acquaintances.
Caregivers had good cause of illness comprehensibility in this study. However, the perceived consequences, emotional, and personal control were low. Regular one on one counselling sessions with caregivers in addition to group sessions in the clinic setting as well as psychotherapy are likely to improve caregivers’ emotional representation of patients’ illness. This will in turn lead to more improvement in patients care by their caregivers.
What is already known on this topic:
What this study adds:
We acknowledge the dedication and contributions of the study subjects, colleagues and nurses for making this study a success.
None.
Self-funded.
Copyright: © 2021 Fatima Bello Jiya., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.