Arie Dian Fatmawati*
Department of Pediatrics, Anna Medika Hospital, Indonesia
*Corresponding Author: Arie Dian Fatmawati, Department of Pediatrics, Anna Medika Hospital, Indonesia.
Received: March 30, 2020; Published: July 30, 2020
Citation: Arie Dian Fatmawati. “Post-Immunization Measles Antibody Levels in Children Aged 1-4 Years”. Acta Scientific Paediatrics 3.8 (2020):30-35.
Background: No study in Indonesia has previously investigated measles antibody levels in children aged 1-4 years by comparing the first and second immunization.
Objectives: We aim to compare the protective measles antibody level after the first and second scheduled immunization.
Method: This cross-sectional study involved six Integrated Service Post (Posyandu) in five Jakarta regions in June-August 2014. Children meeting the inclusion criteria proceeded with measles IgG levels examination. Correlation test assessed the relationship between the second dose of measles immunization and measles antibody levels.
Results: Of 145, 125 subjects (86.2%) reached protective measles antibody levels (≥ 120 mIU/ml). Compared to other age groups, 3-4 years old reported a higher proportion of reaching protective measles antibody levels in 56 subjects (91.8%).
Conclusion: The second scheduled measles immunization provides higher measles antibody levels, with 1.2 times protective levels compared to first-time immunization.
Keywords: Measles Immunization; Measles Antibody Levels; Children Aged 1 - 4 Years
Some developing countries still suffer from measles, especially in Asia and Africa. Data from the World Health Organization (WHO) reported high measles-related mortality worldwide, which amounted to 164.000 in 2008 and 158.000 in 2011. Indonesia is one of 47 measles-prevalent countries in the world[1,2].
Measles could potentially cause an outbreak with a high mortality rate[3-5]. Indonesia’s measles prevalence in 2008-2012 showed a decreasing trend, but outbreaks still often occur[6]. At the beginning of the measles immunization implementation in 1984, measles immunization coverage in Indonesia reached 12.7%, which increased to 85.4% in 1990 and 91.8% in 2004. However, considering seroconversion rate of 85% (the antibodies detected in the serum as a result of infection or immunization) in nine-month-old infants, 91.8% of measles immunization coverage reported in 2004 can only protect approximately 76.5% of infants; where 23.5% others included in the measles-vulnerable groups. Growing numbers of vulnerable groups will potentially lead to a measles outbreak. Therefore, follow-up measles immunization on children under five is of necessity[4,7,8]. In general, outbreaks occurred in several provinces showed the highest prevalence in 1-4 years age groups[9-11].
WHO recommends two-doses measles vaccine administration especially in endemic countries-because 15% of single-dose vaccinated children failed to maintain their immunity[1].To envisage “the world without measles,” as proposed in the Global Measles and Rubella Strategic Plan 2012-2020 as well as supported by WHO and the United Nations of Children’s Fund (UNICEF)[12], the Ministry of Health of the Republic of Indonesia stipulated Regulation of the Minister of Health (Permenkes) RI No. 42 in 2013 concerning follow-up measles immunization at two years of age[13], especially in children not receiving the MMR immunization at 15-18 months old[14].
Two-doses of measles immunization expectedly increase seroprotective factors against measles. Hitherto, no study investigated measles antibody levels following two-doses immunization in Indonesia.
This study aimed to determine the protective measles antibody levels after two-doses immunization (ages 9-12 months and two years of age).
A cross-sectional analytic study conducted in June-August 2014 involved six Integrated Service Post (Posyandu) in five Jakarta regions. Participating in this study were healthy children aged 1-4 years who have acquired first or second-dose measles immunization. Subjects recruited through consecutive sampling by excluding those with measles infection history or immunosuppression (e.g. steroid use > 14 days, suffering from malignancy, autoimmune disease). Children meeting the inclusion criteria had a 3mL blood sample taken by Prodia clinical laboratory officers for measles antibody (IgG) levels examination using the ELISA method. The reagent kit used was Euroimmun AG, D-23560, Lubeck, Germany, Cat: EI2610-9601G, Lot: E140325CA product kit. The WHO Expert Committee on Biological Standardization recommended using the Third International Reference serum as a protective measles antibody reference, i.e. ≥ 120 mIU/ml[15].This study had the Ethics Committee of Health Research approval (certificate of ethical clearance number 712/H2.F1/ETHICS/2013 dated 18 November 2013). Collected data further processed using SPSS version 17.0. The bivariate analysis investigated the relationship between independent variables, i.e. age at measles antibody examination date, age at immunization, nutritional status, health condition during measles immunization, and frequency of measles immunization, with protective measles antibody levels using Chi-squared method (X2). Fisher’s test or cell merging will substitute the Chi-square method if required statistical assumptions not fulfilled.
One hundred fifty-nine children were fulfilling the inclusion criteria. Three subjects dropped-out from this study: two refused blood sampling, and the blood volume of another subject was not sufficient for antibody analysis. Of the remaining 156 research subjects, 11 blood samples lysed and excluded from the analysis. A total of 145 subjects analyzed in this study.
Most subjects (42.1%) were 3-4 years old, female (58.6%), well-nourished (63.4%), and healthy. Subject characteristics as displayed in table 1.
Of 145 subjects, 125 (86.2%) had higher measles antibody reaching the protective level (≥120 mIU/mL), and 20 subjects (13.8%) had measles antibody below the protective level (<120 mIU/mL) (Table 2). In this study, measles antibody levels did not follow the normal distribution, so data presented as a median and minimum-maximum range. Overall, the median of measles antibody levels is 753 mIU/mL. The median of measles antibody levels in protected groups is 844 mIU/mL (129 - 5000 mIU/mL).
Of several subject characteristics, only age at the measles antibody measurement has a significant relationship with the measles antibody levels (Table 3). The age group of 3-4 years had higher measles antibody reaching protective levels (91.8%) compared to the age group of 2-3 years (88.2%) and 1-2 years (72.7%).
Table 1: Subject characteristics.

Table 2: Subject measles antibody levels.
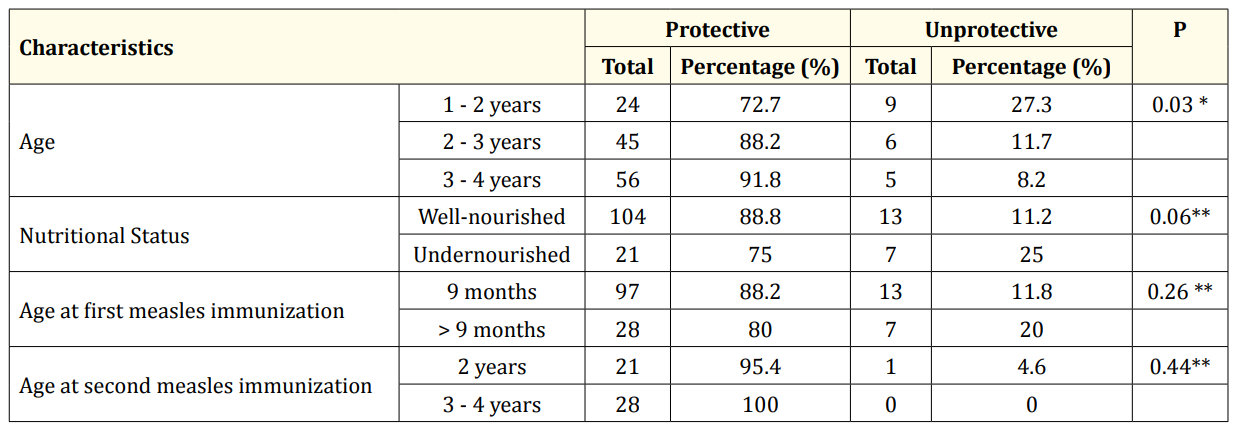
Table 3: Relationship of age, age at measles immunization and nutritional status with measles antibody levels. *Chi-square test; **Cells merging; Fisher’s test; p < 0.05, statistically significant.
Of 95 receiving single-dose measles immunization, 76 subjects (80%) had higher protective antibody levels. While 50 receiving second-dose measles immunization, 49 subjects (98%) had higher protective antibody levels (Table 4).

Table 4: The relationship between measles immunization frequency with measles antibody levels. *Chi-squared test. From test Chi-squared obtained the 1.2 prevalence ratio (95% CI, 1.1-1.4; p = 0.002).
This study shows that most of the subjects (86.2%) had protective measles antibody levels. The presence of post-immunization measles antibody with protective levels received influences from several factors, namely decreasing maternal measles antibody levels, immunological maturity, vaccine dose, and vaccine strain[16]. Some biological factors determine measles vaccine effectiveness and immunogenicity. Immune system immaturity inhibits protective antibody formation, namely limited B-cell production and mechanism of antigen presentation as well as inefficient Th cell[16]. Babies at a young age (≤6 months) do not have sufficient antibody levels after measles immunization with weakened measles vaccines, especially in the absence of maternal antibody. IgG formation response is lower than adults, thus curtails the avidity. Inefficient immune response potentially arises from disrupted interaction between the T-lymphocytes and antigen-presenting cells[15].
More subjects (51.7%) received deltoid measles immunization injection than the anterolateral thigh. Recent literature recommended anterolateral thigh for immunization in infants and children under 12 months[17]. While the deltoid is an alternative for older children (able to walk) and adults. The anterolateral thigh region consists of vastus lateralis muscles and recommended as the injection site for infants and children under 12 months. Such a region is thick enough to absorb the injected vaccine adequately compared to the deltoid area. Anterolateral thigh injection also avoids sciatic nerve injury risk during gluteal injections and thick subcutaneous fat tissue in the anterior thigh. However, children above 12 months may receive measles injection in the deltoid area. No literature suggested immune response differences in either the anterolateral thigh or deltoid injection. To ensure adequate immune response, performing a subcutaneous injection is essential to reach the lymphoid tissue[17].
In this study, most subjects (75.9%) received the first measles immunization at nine months old and second measles immunization at two years old (44%). Age at immunization has a critical influence on the immune response onset. A determinant of the optimal age for measles immunization is a seroconversion rate increase after measles immunization, influenced by the average age at immunization or infection onset[15]. Based on the measles vaccine immunogenicity theory, the proportion of children forming a protective measles antibody is 89.6% if immunization carried out at 8-9 months, 92.2% at 9-10 months, and 99% at 11-12 months[16]. Measles vaccine-induced antibody response proportionally increases with age up to 15 months, alongside decreasing maternal measles antibody and matured immune system. Maternal measles antibody inhibits viral replication in the weakened vaccine in eliciting an immune response. Antibody avidity is also a vital characteristic of a mature antibody response defining the bonding strength of antibodies to measles antigens.
The presence of high-avidity antibody response enhances protective measles immunity. Antibody avidity to the weakened vaccine is usually lower in children immunized at six or nine months compared to children immunized at 12 months[15]. As such, first dose measles immunization will be more efficient in forming antibodies to reach the protective level when given at 12 months of age. However, the first dose measles immunization administered at nine months does not harm, and per the WHO recommendations, considering Indonesia as one of the high-measles-transmission countries[12].In areas with high transmission, measles may infect the young population, so the optimal strategy would require early measles immunization, starting at nine months of age. On the contrary, in low-measles-transmission areas, the immunization can delay until 12 months or older[15].
This study observed a relationship between measles immunization frequency with the onset of protective antibody levels, where the prevalence ratio (PR) was 1.2 (95% CI, 1.1-1.4; p=0.002). Such a finding suggests the re-vaccinated population has 1.2 times higher probability of reaching protective measles antibody levels. Follow-up measles vaccination intended to immunize children failing to respond on the first immunization and those without previous measles vaccination history. The immunologic outcome on re-vaccination is reliant upon immune response adequacy after first-dose immunization. With second-dose measles vaccine given to children one year or older who failed to reach protective antibody levels after first-dose vaccination, most will achieve protective antibody levels[15].
The proportion of children aged 1-4 years with protective measles antibody levels after first-dose immunization is 80%, where a median of antibody levels is 733,5 mIU/mL. Meanwhile, the proportion of children aged 1-4 years with protective measles antibody levels after second-dose measles immunization is 98%, where a median of antibody levels is 885 mIU/mL. Age of measles antibody level examination is the only determining factor of the emergence of protective measles antibody level, while age of immunization dan nutritional status have no role. Second-dose immunized subjects have higher protective measles antibody as much as 1.2 times compared to first-dose immunized subjects.
Copyright: © 2020 Arie Dian Fatmawati. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.