Ma Kariza V Pabelonio, Elynn L Go and Lorela L Cortez-Dy*
Department of Pediatrics, Las Piñas Doctors Hospital, Las Piñas, Philippines
*Corresponding Author: Lorela L Cortez-Dy, Department of Pediatrics, Las Piñas Doctors Hospital, Las Piñas, Philippines.
Received: March 12, 2020; Published: June 23, 2020
Citation: Lorela L Cortez-Dy., et al. “The Relationship between Cigarette Smoking with Risk Taking Behaviour in Adolescents Ages 11 - 18 at a Public High School in Las Piñas City Using the CRAFFT Screening Tool”. Acta Scientific Paediatrics 3.7 (2020):64-75.
Background: Risk taking, to some extent, is a part of the development of an adolescent. Trying new things or experimentation are behaviours used to discover their independence as well as their identity. But some risk taking behaviours are health compromising and should be recognized early. The CRAFFT screening tool was developed to measure these behaviours to be able to gauge a level of surveillance for a child.
Objective: To determine the relationship between cigarette smoking with risk taking behaviour in adolescents ages 11 - 18 at a public high school in Las Piñas City using the CRAFFT screening tool.
Method: A cross-sectional study design. Purposive sampling of 615 students from an anonymous public high school in Las Piñas was done. Subjects were asked their age, sex and year level and answered a questionnaire called the CRAFFT screening tool to measure risk-taking behaviour. Z-test was used to test the proportions of the variables. Chi-square was used to test the association of smoking in the risk taking behaviour of cigarette smokers versus non-cigarette smokers.
Results: Participants were a total of 615. 36.1 percent of the sample population were grade 7 students, predominated by males at 56.7 percent, mostly between 15 - 16 years old at 35 percent. 111 out of 615 were found out to be cigarette smokers and is prevalent in grade 10. In relationship of smoking with risk taking behavior, for all grade levels and for both males and females, smoking is associated with risk taking behavior. As for the age, smoking is associated with risk taking behavior in adolescents’ ages 13 - 16, however, there is no association with risk taking behavior for ages 11 - 12 and 17 - 18.
Conclusion: Smoking has an association with risk taking behaviour determined by the CRAFFT questionnaire. This excludes smokers at the age of 11 - 12 and 17 - 18 wherein smoking had no association with risk taking behaviour.
Keywords: Adolescent Cigarette Smoking; Risk Taking Behaviour; CRAFFT Screening Tool; CRAFFT Questionnaire
“The Philippines remains to be Southeast Asia’s second largest tobacco consumer if young Filipinos are not stopped from smoking” - warns the New Vois Association of the Philippines (NVAP). The World Health Organization, along with other countries identifies the Philippines as one of the major tobacco users in Southeast Asia. According to the Global Youth Tobacco Survey (GYTS), more than one in four Filipino children aged 13-15 are smokers. Among those in this age group who smoke, 17.5 percent are girls and 28.3 percent are boys. For smokers aged 16 - 17 years, 25.6 percent are males and 8.1 percent are females. This does not include children of this age group who are exposed to second hand smoke either at home or in public places. It is estimated that 55 percent of Filipino youth are exposed to second hand smoke at home while 65 percent get it in public places [1].
According to the tobacco atlas, most regular smokers initiate smoking before 20 years of age. The youth may have several reasons for starting tobacco use, this includes looking ‘cool’, ‘mature’, or ‘sociable’, or believing that tobacco use is good for coping with stress and weight control. Other reasons may vary across countries, but some common factors are: tobacco use by parents or peers; exposure to tobacco advertising; acceptability of tobacco use among peers or in social norms advertised in movies or tobacco commercials; having depression, anxiety, or stress; and higher accessibility and lower prices of tobacco products [2].
According to WHO on the health effects of smoking among young people, the short-term health consequences of smoking include respiratory and non-respiratory effects, addiction to nicotine, and associated risk of other drug use. Long term health consequences of youth smoking are reinforced by the fact that most young people who smoke regularly continue to smoke throughout adulthood [4]. Teens who smoke are three times more likely than non-smokers to use alcohol, eight times more likely to use marijuana, and 22 times more likely to use cocaine. Smoking is associated with a host of other risky behaviours, such as fighting and engaging in unprotected sex [3].
Tobacco pricing and stronger regulations are crucial to addressing the youth tobacco epidemic. Teens are particularly sensitive to tobacco pricing; Increase of prices or the sin tax prevent many of them from becoming regular tobacco users. The percentage of youth smokers who usually obtain tobacco products in a store is high in many countries, but it can be reduced by banning tobacco product sales to minors or enforcing the existing bans. The minimum legal sale age for tobacco products in several countries is now 21 years [5], which is more effective in reducing youth exposure to tobacco products than is the 18-years limit in effect in the Philippines. Another way was the graphic pictures that came with the cigarette boxes to increase awareness. Apart from the health warning that comes with each box, a helpline from DOH is included for smokers who want to quit.
Risk taking, to some extent, is a part of the development of an adolescent. Trying new things or experimentation are behaviours used to discover their independence as well as their identity and this differs in each stage of development. For early adolescence (10 - 13 years old), self-concept and identity formation is centered in body appearance because this is the time when secondary sex characteristics initiate, and exploration of boundaries for independence and dependence set in. There is little or no regard for interests, beliefs, or attitudes other than one’s own or, there is egocentricity. But this group still follows rules to avoid punishment. Peer affiliation is usually of the same sex but, can be more involved with their peers during middle adolescence (14 - 17 years old). In middle adolescence, emotions are usually the drive of decision making, a sense of invulnerability, a struggle for greater autonomy from the parents, preoccupation with peer culture, and testing the ability to attract a partner that leads to relationships and possibly, sexual activity, which makes this age group the most susceptible to risk taking behaviour. In late adolescence (18 - 21 years old), they are future oriented, are able to think things through independently with improved or lessened impulse control, they are able to distinguish law from morality, has stronger sense of self identity and, peer group and values recede in importance [6].
Some risk taking behaviours are more health compromising. According to the organizations that were created by the WHO as well as our own country’s surveillance on the risk taking behaviour of the youth today, two out of three 13 - 15 years old high school students in the country, had a drink of alcohol other than a few sips admitted that they started drinking alcohol before 14 years old. More boys at 20 percent than girls at 16.6 percent are current alcohol drinkers or had at least one drink of alcohol on at least one day within 30 days prior to conduction of their survey. Boys at 18.6 percent, more than girls at 14.4 percent drank so much alcohol, had experienced to be really drunk, one or more times during their life. More than one in ten or 10.1 percent of the 13 - 15 years old high school students used drugs. Males 12.3 percent, more likely than females 8.1 percent. Similarly, a higher proportion of males than females used marijuana males at 8.6 percent, females at 5.3 percent or amphetamines/methamphetamines, males at 6.1 percent, females at 3.5 percent one or more times during their life. Among students that used drugs, a total of 77.7 percent of high school students reported that their first drug use was before age 14 years. The females 83.0 percent are more likely than males 74.5 percent to have used drugs for the first time before they turned 14 years old. Almost 6 out of 10 fourth year high school students used drugs, have initiated drug use before 14 years old (GSHS 2015). Other risk taking behaviour enumerated were as follows: 23.5 percent of young people had premarital sex (YAFS3), 2 percent of sexually transmitted infections are in the 13-17 year old age group, 2 percent of HIV/AIDS are 10-19 years old (Philippine AIDS Registry), 22.3 percent of maternal deaths were women < 24 years old (Philippine Health Statistics 2003), and 16.7 percent of youth considered suicide (GSHS 2007) [7]. There is also an increasing trend of vehicular accident deaths since 2006. According to the Philippine Statistics Authority, for 2015 there were 9,994 deaths due to vehicular accidents, from ages 10 - 14, 230 deaths and for 15 - 19, 826 deaths. The number one cause is texting while driving followed by driving under the influence of alcohol [12].
This study focuses on substance use. It is one of the most common health risk behaviour among adolescents and is one of the greatest threats to their current and future health. In the Philippines, in the war against drugs, from July 1 to August 28, 2017, 20,584 minors ages 11 - 18 have surrendered to local police offices, according to the Philippine National Police’s Women and Children Protection Center. 98 percent of these minors admitted to being drug users, while only 1.33 percent surrendered as drug pushers or sellers and the remaining 0.67 percent were runners. 45.43 percent were from high school. These are alarming numbers, and these numbers would just be increasing if do not do something about it [8].
The Department of Health (Philippines), in its Adolescent and Youth Health Policy (2000), identified risk taking behaviour that poses health risks are: substance abuse, premarital sex, early childbearing, abortion, HIV/AIDS, violence, accidents, malnutrition, and mental health.
In the Philippines, children are often used in drug related activities, maybe as couriers or front personnel to reduce suspicion from the authorities, and, in some buy-bust operations, some of these children are slain. In a position paper from the Philippine Pediatric Society, they addressed that drug addiction is not just a criminal issue and should be dealt with holistically. Aside from the random drug testing implemented by the government, other solutions were enumerated such as: 1) working with family systems and values, improving parent child communication, providing drug education, rule setting and parental monitoring and supervision. 2) Early detection of risk factors like academic failure, early aggression, and school dropout, to be addressed by schools and communities. 3) In adolescents, drug education, competence in drug resistance skills and reinforcement of antidrug attitudes and strengthening personal commitments against drug use. 4) Consistent messages delivered through a concerted effort by the community - families, schools, barangay leaders and faith-based organizations.
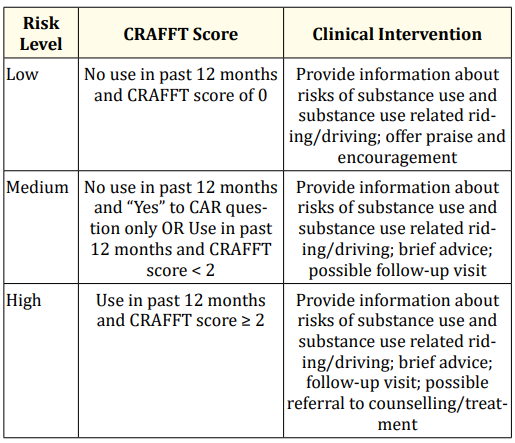
The CRAFFT screening tool was developed by Dr. Knight., et al. at the Centre for Adolescent Substance Abuse Research (CeSAR) at Boston’s Children’s Hospital in the United States of America. Their objective was to develop an assessment tool like the CAGE - a questionnaire for alcoholism, it is an acronym for 1) C - cut or cutting down on alcohol 2) A is for annoyed by people criticizing their drinking, 3) G for feeling bad or guilty for drinking, 4) E for eye opener, drinking first thing in the morning. The CAGE is used in adults for detecting alcoholism. But unlike the CAGE, the CRAFFT was designed to be developmentally appropriate for adolescents (12 - 21 years old) and screen conjointly for both alcohol and drug use because, alcohol-and drug-related-motor-vehicle crashes are the leading cause of death among adolescents in the United States. CRAFFT is an acronym for C-car or if an adolescent drives or has been driven by someone under the influence; R-relax, if an adolescent uses substances such as alcohol or drugs to unwind; A-alone, if an adolescent uses alcohol or drugs when they are alone; 1st Fforget, if an adolescent forgets things while using alcohol or drugs; F-family or friends, if family or friends ever advised them to cut down on using alcohol or drugs; T-trouble, if the adolescent had ever gotten in trouble while using drugs or alcohol.
The CRAFFT screening tool was originally designed to screen adolescents at high risk of substance use disorders in primary medical care offices. However the necessity for an adolescent screening measure was made apparent by research findings suggesting that half of high school students drink, a third binge drink, and a fourth use marijuana. Findings like these also contributed to the identification of a need for a tool like CRAFFT to be developed. It is has a scoring system as well as the corresponding intervention as follows [9]:
In a study done by D’Amico., et al. regarding the best way to identify risk youth for substance abuse, they had compared the psychometric performance of 4 screeners namely: National Institute on Alcohol Abuse and Alcoholism Screening Guide (NIAAA SG), CRAFFT, The Personal Experience Screening Questionnaire Problem Severity Scale (PESQ-PS) and Alcohol Use Disorders Identification Test (AUDIT). The PESQ-PS and CRAFFT (97 percent Sensitivity) had performed better than the NIAAA SG (87 percent Sensitivity) and AUDIT (70 percent Sensitivity) [10].
There are two versions of the CRAFFT screening tool: A clinician interview and a self-administered questionnaire. Research has found that adolescents report greater comfort and likelihood of honesty with self-administered questionnaires. It is also more time efficient to administer than an interview. The most important principle is to ensure that the parents cannot see their children’s responses, so that adolescents feel comfortable reporting honestly. In a study done by Dr. Knight., et al. in the adolescents’ preference for substance abuse screening in primary care practice, participants between 12 - 18 years old were given the CRAFFT test by interview from a nurse, a doctor, and a self-administered questionnaire via the computer and paper. Paper was the screening administration method most preferred with a mean rank of 2.92 (95 percent CI 2.87 - 2.96), second was the computer, third was the nurse and last was the doctor. The findings were similar for participants reports of being “very likely” to be honest when answering substance abuse screening questions [9].
Is there a relationship between cigarette smoking with risk taking behaviour in adolescents ages 11 - 18 at a public high school in Las Piñas City using the CRAFFT screening tool?
Where: Hø (null hypothesis) = there is no a relationship between cigarette smoking with risk taking behaviour in adolescents ages 11-18 at a public high school in Las Piñas City using the CRAFFT screening tool.
Hꭤ (alternative hypothesis) = there is a relationship between cigarette smoking with risk taking behaviour in adolescents ages 11-18 at a public high school in Las Piñas City using the CRAFFT screening tool.
One of the major problems in the Philippines is tobacco use or cigarette smoking. Aside from the health issues that come along with it, this study aims to determine if there is a relationship with smoking and risk taking behaviour, particularly on drug use, by using the CRAFFT questionnaire. From the ways enumerated by the Philippine Pediatric Society in dealing with drug use holistically, this study with come into early detection. This research can open the way to use of another tool in screening children for risk taking behaviour apart from the random drug testing, to guide parents and guardians in the surveillance of their young to lessen the prevalence of risk taking behaviour that compromises an adolescent’s health.
In 2017 the creators of CRAFFT had released a manual that included nicotine use called the CRAFFT+N, both questionnaire and clinician interview. Nicotine use is also considered a risk taking behaviour. However, from the CeSAR’s publication in adolescent health, there were no studies which supported the use of nicotine as part of the risk taking behaviour in CRAFFT hence, this study aims to support the association of nicotine use with risk taking behaviour.
To determine if there is a relationship between cigarette smoking with risk taking behaviour in adolescents ages 11 - 18 at a public high school in Las Piñas City using the CRAFFT screening tool.
Study design: A cross-sectional study.
Description: There are a total of 1077 students in the public school chosen for the study. 312 students from grade 7, 312 students from grade 8, 232 students from grade 9, 221 students from grade 10.
583 students are male, 494 students are female.
Inclusion: Purposive sampling was employed among 615 high school students out of 1077, ages 11 - 18 years old studying in an anonymous public school in Las Piñas SY 2018 - 2019.
Exclusion: Students that are less than 9 years old and more than 19 years old. Four (4) students were excluded due to age more than 19 years old.
Sample Size: Recommended sample size is 284 participants however, to decrease margin of error all 615 students were included.
N = Population size
e = Margin of error
z = z score the number of standard deviations a given proportion is away from the mean which is (1.96) or a 95% confidence level.
The survey was distributed concealed in a brown envelop to the participating students grades 7, 8, 9 and 10 in a public high school in Las Piñas. Subjects were first asked to answer a portion of the survey where they had to write their name (which was optional), age, sex, year level, and if he or she is a cigarette smoker or a non-cigarette smoker. The next part was the CRAFFT questionnaire. Each class took 10 to 15 minutes to answer the survey and questionnaire.
After consolidation of data using Microsoft Excel, z-test was used to test the proportions of the variables. Chi-square was used to test the association of smoking in the risk taking behaviour of cigarette smokers versus non-cigarette smokers.
This study is focused on public high school students, grades 7 to 10, ages 11 - 18 and the level of risk taking behaviour measured by using the CRAFFT questionnaire. Subjects are studying in an anonymous public high school in Las Piñas school year 2018 - 2019. The research was conducted during August to September 2018.
The general purpose of this study is to know if there is a relationship between cigarette smokers with risk taking behaviour and to compare it with non-cigarette smokers.
The ethics committee of the Las Piñas Doctors Hospital approved of the study. Consent was secured and the participants’ identity was undisclosed to preserve confidentiality.
Table 1 shows the participants’ profile. In terms of grade, the highest number of participants are Grade 7 students (36.1%) and Grade 10 students (31.1%). Majority of the participants are males at 56.7%. Students aged 15 - 16 years represent the highest proportion of students in terms of age.
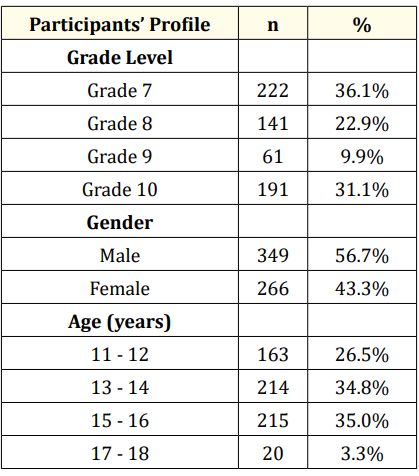
Table 1: Participants profile (N = 615).
The smoking status of the students in terms of grade level, gender and age is shown in table 2. Overall there are 111 out of 615 cigarette smokers or 18 percent from the participants. In Grade 7 and Grade 10 students, there is a significant difference (p < 0.05) in the proportions of smoking status. For Grade 8 and Grade 9 students, the proportion of smokers to non-smokers are relatively the same (p > 0.05). Smoking is significantly more prevalent among Grade 10 students while non-smoking is significantly more prevalent among Grade 7 students.
In terms of gender, there is a significant difference in the proportions of smoking status. Smoking is significantly prevalent among males while non-smoking is significantly prevalent among females.
In terms of age, there is a significant difference in the proportions of smoking status among students aged 11 - 12, 15 - 16 and 17 - 18 years while the proportion of smokers to non-smokers are relatively the same among students aged 13 - 14 years. Smoking is significantly more prevalent among students aged 15 to 18 years while non-smoking is more prevalent among students aged 11 to 12 years.
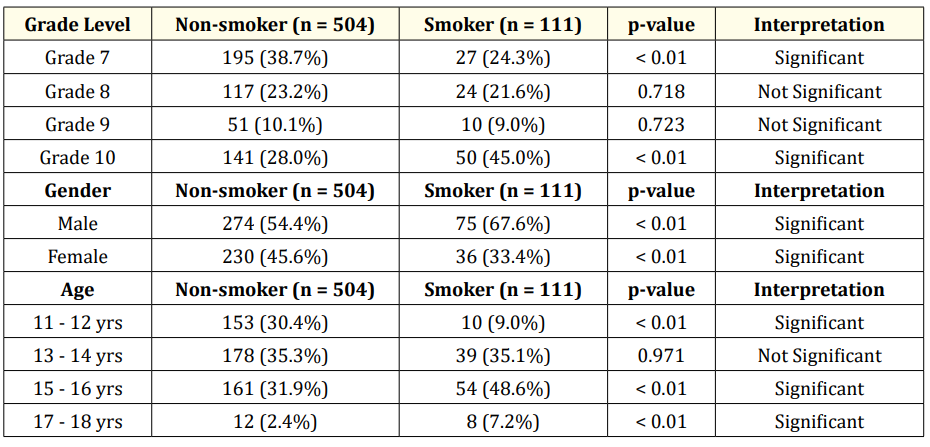
Table 2: Smoking status. *P-value of < 0.05 is significant.
The risk taking behavior of the students in terms of grade level, gender and age is shown in table 3. Only Grade 9 students indicated relatively the same risk taking behavior. Among Grade 7, Grade 8 and Grade 10 students, there is a significant difference in the proportions of risk taking behavior. Medium and high risk taking behavior is significantly more prevalent among Grade 10 students while medium risk taking behavior is significantly more prevalent among Grade 7 students and low risk taking behavior is significantly more prevalent among Grade 7 and among Grade 8 students.
The risk taking behavior of the students when it came to gender, among Grade 7 students, there is a significant difference in the proportions of proportions of risk taking behaviors. Low and medium risk taking behavior is more prevalent among male and among female students.
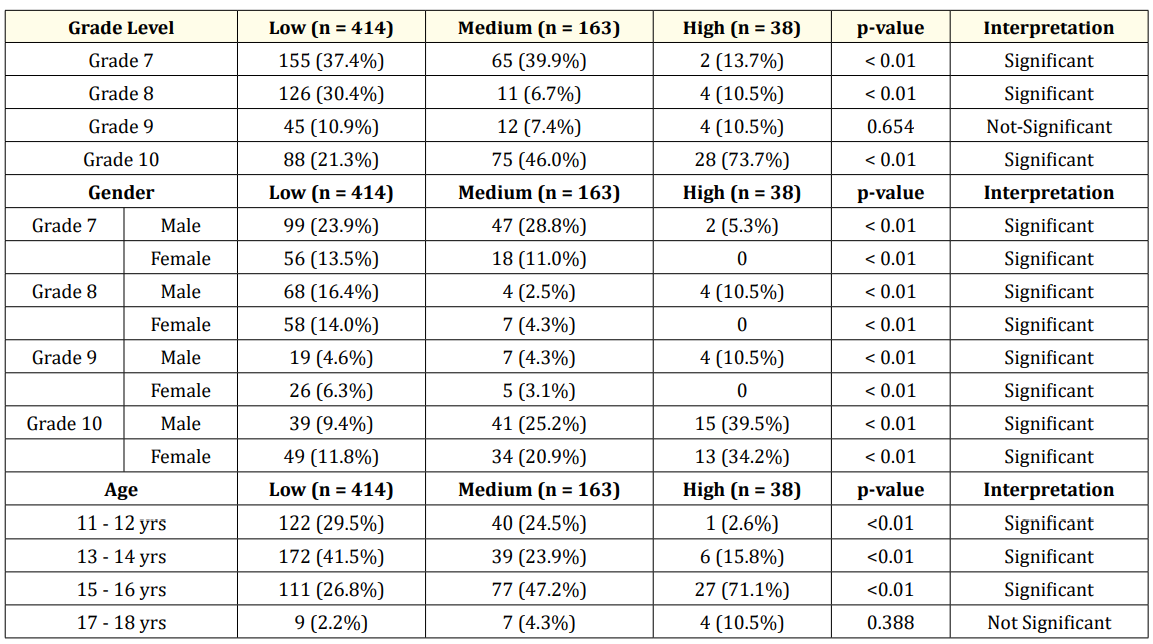
Table 3: Risk taking behavior. *P-value of < 0.05 is significant
Among Grade 8 students, there is a significant difference in the proportions of risk taking behaviors. Low and high risk taking behavior is significantly more prevalent among male students while low risk taking behavior is significantly more prevalent among female students.
Among Grade 9 students, there is a significant difference in the proportions of risk taking behaviors. High risk taking behavior is significantly more prevalent among male students while low risk taking behavior is significantly more prevalent among female students.
Among Grade 10 students, there is a significant difference in the proportions of risk taking behaviors. Medium and high risk taking behavior is significantly more prevalent among male and among female students.
In risk taking behavior of the students when it came to age, there is a significant difference in the proportions of risk taking behavior among students aged 11 - 12, 13 - 14 and 15 - 16 years while the proportions of risk taking behavior among students aged 17 - 18 years are relatively the same. Among students aged 11 - 12 years, low and medium risk taking behavior is significantly more prevalent while among students aged 13 - 14 years, low risk taking behavior is significantly more prevalent and among students aged 15 - 16 years, medium and high risk taking behavior is significantly more prevalent.
The association between smoking status and risk taking behavior of the students in terms of grade level, gender and age is shown in table 4. There is a significant association (p < 0.01) between smoking status and risk taking behavior among students in each grade level. Smoking status is significantly indicative of risk taking behaviors of students in each grade level.
In terms of gender, there is a significant association (p < 0.01) between smoking status and risk taking behavior among male and female students. Smoking status is significantly indicative of risk taking behaviors for male and female students.
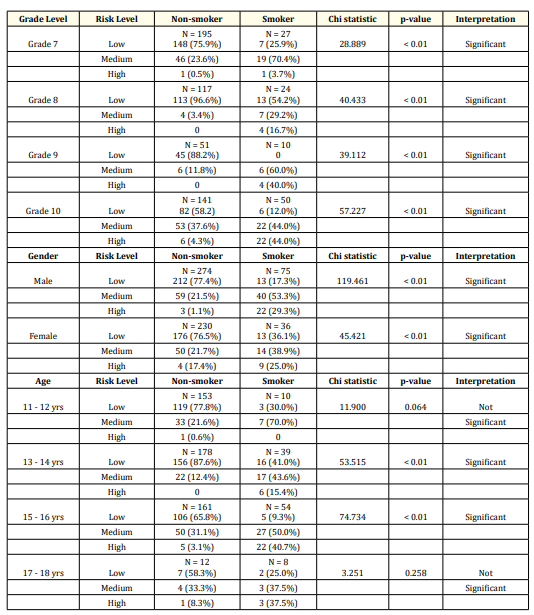
Table 4: Association between smoking status and risk taking behavior. P-value of < 0.01 is significant.
In terms of age, there is no significant association (p > 0.05) between smoking status and risk taking behavior among students aged 11 - 12 years and among students aged 17 - 18 years. Smoking status is not indicative of risk taking behaviors for students in these age groups.
However, there is a significant association (p < 0.01) between smoking status and risk taking behavior among students aged 13 - 14 years and among students aged 15 - 16 years. Smoking status is significantly indicative of risk taking behaviors for students in these age groups.
The study had a total of 615 participants. Highest number of subjects were from grade 7 at 36.1 percent, 22.9 percent were from grade 8, 9.9 percent were from grade 9 and from grade 10, 31.1 percent. When grouped by gender, the participants are predominantly male at 56.7 percent, females were the remaining 43.3 percent. When grouped according to age, majority are 15 - 16 years of age at 35 percent, for 13 - 14 years old 34.8 percent, 11 - 12 years old 26.5 percent, and for 17 - 18 years old, the remaining 3.3percent.
The smoking status of the students is shown in table 2. Overall there are 111 out of 615 cigarette smokers or 18 percent from the participants. Among Grade 7 and Grade 10 students, there is a significant difference (p < 0.05) in the proportions of smoking status. For Grade 8 and Grade 9 students, the proportion of smokers to non-smokers are relatively the same (p > 0.05). Smoking is significantly prevalent among Grade 10 students while non-smoking is significantly prevalent among Grade 7 students. Non-smoking was prevalent among female students at 45.6 percent (p < 0.01) and smoking was significantly prevalent male students at 67.6 percent (p < 0.01). In terms of age, smoking was significantly prevalent among students aged 15 - 16 at 48.6 percent and 17 - 18 years at 7.2 percent (p < 0.01), while non-smoking was prevalent among students aged 11 to 12 years at 30.4 percent (p < 0.01). There are a number of reasons for starting tobacco use and according to the tobacco atlas, the child might want to look “cool,” “mature,” or “sociable,” or believes that tobacco use is good for coping with stress and weight control [2]. The result of this study however, was in contrary to the Global Youth Tobacco Survey in 2015 which is more than one in four Filipino children aged 13 to 15 are smokers. It is possible that the numerous health regulations against smoking had taken effect. The study was still consistent with males as predominant user of tobacco at 67.6 percent. Reasons for initiation varies across nations but common factors are tobacco use of parents or peers - it is estimated that 55 percent of Filipino youth are exposed to second hand smoke at home while 65 percent get it in public places [1]. Children see these actions thinking it is acceptable because adults, or the people they look up to, the people they are with everyday are smoking, and the lack thereof of their knowledge, their innocence and curiosity, a habit can be born. Depression, anxiety and stress can also be a cause. Mental health problems can initiate tobacco use because of the need to search for comfort. Some of these children turn to food, alcohol or drugs and another thing they find solace in is through smoking. Also, being that the Philippines is a third world country, we have higher accessibility to tobacco products because apart from the age limit, which is 18 years old compared to other countries that sells to 21 years old and above, the Philippines still has lower prices of tobacco products compared to other countries [5].
For risk taking behavior as determined and scored by using the CRAFFT screening questionnaire, The risk taking behavior of the students in terms of grade level is shown in table 3. Only Grade 9 students indicated relatively the same risk taking behavior (p 0.654). Among Grade 7, Grade 8 and Grade 10 students, there is a significant difference in the proportions of risk taking behavior (p < 0.01). Medium and high risk taking behavior is significantly prevalent among Grade 10 students while medium risk taking behavior is significantly prevalent among Grade 7 students and low risk taking behavior is significantly prevalent among Grade 7 and among Grade 8 students. When grouped according to gender shown in table 4, in grade 7 students both low and medium risk taking was prevalent among male and female students (p < 0.01). In grade 8, low and high risk taking behavior was prevalent among male students (p < 0.01), while low risk taking behavior was significantly prevalent among female students (p < 0.01). In grade 9 students, high risk taking behavior was prevalent among male students (p < 0.01), while low risk taking behavior was significantly prevalent among female students (p < 0.01). For grade 10, medium and high risk were both prevalent among male and female students (p < 0.01). Medium and high risk taking is predominantly male... More boys are currently alcohol drinkers at 20 percent compared to the girls at 16.6 percent. Boys tend to get drunk at 18.6 percent compared to the girls at 14.4 percent. More males have used drugs at 12.3 percent more likely than females at 8.1 percent. Males have constantly been associated with higher risk taking behavior than females [6]. In terms of age as shown in table 3, for students 11 to 12 years old, low and medium risk taking behavior was prevalent (p < 0.01) and in 13 to 14 years old, low risk was significantly prevalent (p < 0.01).This age group belongs in early adolescence. Their milestones include initiation and exploration of boundaries in independence and dependence. This is the time when they are testing the limits… “What are the rules that are firm and what rules can they bend?” This is the start of transition from childhood to adolescence. What also begins is the risk taking. But seeing as low and medium risk taking is more prevalent in this age group, it can be explained by their ability to conform more than other age groups. This is still the stage wherein, they follow the rules to avoid being punished because there is still a level of dependence with their parents. In 15 to 16 years medium and high risk taking behavior were more prevalent. This age group belongs to middle adolescence. In middle adolescence, there is a struggle for greater autonomy from the parents, in decision making, emotions are usually the drive. There is also sense of invulnerability. They are more preoccupied with peers, and they spend less time with family. This is also the period wherein they test the ability to attract a partner. Attracting a partner leads to relationships, and these relationships may lead to sexual activity, which makes this age group the most susceptible to risk taking behaviour. In late adolescence (18 - 21 years old), milestones include the ability to think things through independently, they are future oriented, able to distinguish law from morality, peer groups recede in importance, there is improved impulsivity and they have stronger sense of self-identity. This can explain why in adolescents aged 17 to 18, there was no significant difference in proportions of risk taking behavior or, it was relatively the same (p 0.388). Self-identity is composed of relatively permanent self-assessments, such as personality attributes and knowledge of one’s skills and abilities. Self-identity becomes more concrete after the experimentation and the experiences they go through that makes an impact on their lives [6].
In the association between smoking status and risk taking behavior of the students in terms of grade level shown in table 4, there is a significant association (p < 0.01) between smoking status and risk taking behavior among students in each grade level. Smoking status is significantly indicative of risk taking behaviors of students in each grade level. This can be explained by the variety of age groups per grade level. There are students in the 7th, 8th and 9th grade that are 15 - 18 years old, it is possible that some of them had started late in high school due to financial problems or has trouble keeping up with grades. In the association between smoking status and risk taking behavior of the students in terms of gender, there is a significant association (p < 0.01) between smoking status and risk taking behavior among male and female students. Smoking status is significantly indicative of risk taking behaviors for male and female students.
According to age, there is a significant association (p < 0.01) between smoking status and risk taking behavior among students aged 13 - 14 years and among students aged 15 - 16 years. Smoking status is significantly indicative of risk taking behaviors for students in these age groups. However, there is no significant association (p > 0.05) between smoking status and risk taking behavior among students aged 11 - 12 years and among students aged 17-18 years. Smoking status is not indicative of risk taking behaviors for students in these age groups. For age 11 - 12, since they conform more to rules to avoid being punished, they are more cautious than teenagers from middle and late adolescence. This age group has smokers but risk taking is low to medium. As for students aged 17 - 18, they have stronger self-identity, they are able to think things through and have better concept of what they like and do not like. There is risk taking in this age group, but is not limited to smoking. Adolescents at this age can be smokers but are not risk takers, or are non-cigarette smokers but uses drugs or alcohol.
Table
This study demonstrated that cigarette smoking has a relationship with risk taking behaviour in adolescents aged 11 - 18. (A) The study had a total of 615 participants. Highest number of subjects were from grade 7 at 36.1 percent, predominantly male at 56.7 percent, majority are 15 - 16 years of age at 35 percent. (B) There are 111 out of 615 cigarette smokers or 18 percent from the participants. There is a significant difference in the proportions of smoking. Smoking is significantly prevalent among grade 10 students, male, ages 15 - 18 years. Non-smoking on the other hand is significantly prevalent among grade 7 students, females and with students between 11 - 12 years old. (C) There is a significant difference in the proportions of risk taking behavior. Medium and high risk taking behavior is significantly more prevalent among grade 10 students, male and ages 15 - 16 years old, while low risk taking behavior is significantly more prevalent among Grade 7 and 8 students, female and, between ages 11 - 12 years old. (D) There is a significant association between smoking status and risk taking behaviour in each grade level, both male and female and students between 13 - 16 years old. Smoking status is significantly indicative of risk taking behaviours. There is no significant association between smoking status and risk taking behaviour for ages 11 - 12 and 17 - 18.
Nicotine use is included in the list of risk taking behaviours. It was found out that as early as 11 years old, adolescents use or experiment with substances such as nicotine, alcohol and drugs. It is recommended that we use the CRAFFT+N self-administered questionnaire in early adolescence in order to gauge a level of surveillance in a child. A self-administered questionnaire is cost effective and time saving, answering the questionnaire took 10 - 15 minutes per class. The CRAFFT not only detects risk taking behaviour but is also used in reaching a diagnosis for substance abuse. After determining the level of risk taking behaviour reciprocates to an intervention to discourage and protect the child from repeated use of harmful substances.
For future studies, we can include other variables in the demographic profile, for example, the social economic status, educational attainment of the subject’s guardian. For further exploration of the topic, other populations may be studied, for example, students from private schools, private versus public, adolescents from rural versus urban places, or smoking versus exposure to second hand smoke versus non-smokers and the like.
The researcher acknowledges that this study could not have been possible without guidance from the co-authors Dr. Elynn Go and Dr. Lorela Cortez-Dy, they were there from conceptualization and seeing this study through to the end. The researcher would also want to thank the efforts of the teachers in the school who helped her administer the questionnaires, the children who participated, and the principal who allowed us to conduct the study in their humble school and, to Mr. John Calumno, the statistician, for consolidating the results of this study. I would also like to thank my family, first and foremost my parents Mr. Edward Pabelonio and Mrs. Erlinda Pabelonio for the support they have given me all throughout my life and, Dr. Mikhail Jorex Oraa for strength that he has provided me to finish this study. This research is most especially dedicated to God. I lift this all up to Him and thank Him for the opportunity to contribute knowledge in the field of adolescent medicine.
Copyright: © 2020 Lorela L Cortez-Dy., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.