C A Gopalakrishna Mithra, Chikkanarasareddy PS, Anjanamurthy, Gaythri Devi C and Basavarajaiah DM*
Department of Pediatrics, Bangalore Medical College and Research Institute, Bangalore, India
*Corresponding Author: Basavarajaiah DM, Department of Pediatrics, Bangalore Medical College and Research Institute, Bangalore, India.
Received: March 09, 2020; Published: May 31, 2020
Citation: Basavarajaiah DM., et al. “Prevalence of Type-II Diabetics in Children”. Acta Scientific Paediatrics 3.6 (2020):45-48.
According to the NIHFW (2015) and CDC (2011) reported that type II diabetes is a scourge, an approximately 430 children were suffering from the type II diabetes between age group 10 - 19 years. Type II diabetes is a long-term illness that can lead to serious complications if person does not receive treatment. At the moment, there is no cure. However, with a carefully controlled diet, lifestyle modification and medication to control blood sugar, the disease can enter long term remission. In this present research study we estimate the prevalence of type-II diabetes in children and their risk factors for the intervention of type-II diabetes. Retrospective observational study was conducted at Department of Paediatrics, Bowring and Lady Curzon Hospital, Bengaluru for the period of (2015 - 2017). Then cases were screened in OPD and cases admitted ward. The inclusion and exclusion criteria were employed to screening of patients. Demographic and risk parameters were collected tested questionnaires. Collected data were analysed by using Minitab. The results describe, the mean age of the type II exposed cases was 13.45 years with SD 2.11 years (IQR 9 - 17 Years); the mean BMI was 36.22 kg/m2 , height to weight ratio was found to be significantly associated with type II diabetes. Risk factors significantly differ with increase of type II diabetes, intake of frozen food, junk food, family history, sedentary life, family separation, obesity fell in to the body mass index condition is the toll to increase the prevalence of type II diabetes. The results conclude that, practice of controlled diet, physical exercise, encourage the children on positive support of academic, physical exercise activities, allow to positive thinking will be the key indicators for reducing the number of infectives of type II diabetes.
Keywords: Type-II Diabetic; Community Level; Demographic Risk Factors
As per the WHO, south Asian countries like India and developing countries type II diabetes in children are a chronic disease that affects the way child’s immune system processes sugar. Without any treatment intake, the disorder causes sugar build up in the blood, which can lead to serious long-term consequence we faced in the children. In type 2 diabetes, the cells in a child's body are resistant to the effects of insulin and glucose builds up in the bloodstream. Eventually, this causes glucose to reach dangerous levels in the body. The exact cause of type II diabetes is unknown. Past Literature revealed that, the family history and genetics appear to play an important role [1,2]. Inactivity and excess fat fell on BMI 95th percentile also seem to be important factors for diabetes type-II in children [3]. By the year 2050, one in three people will have diabetes. Children from certain racial and ethnic groups are at higher risk, including African American, Hispanic/Latino, Asian/Pacific Islander and Native American children. Children and teens may be able to prevent diabetes or delay its onset for many years [4]. Small changes can make a big difference. Even a small amount of weight loss can help prevent or delay diabetes [5,6]. Children and teens with type 2 diabetes often feel no symptoms at all. However, be aware of some common symptoms of type 2 diabetes. Increased thirst frequency or night-time urination, blurry vision unusual fatigue. The risk factors of type-II diabetics include overweight, family history of diabetes, female gender, specific ethnic groups (American Indian, African-American, Asian, or Hispanic/Latino), other problems with insulin resistance (most people with type 2 diabetes in childhood are diagnosed at the start of puberty, a developmental stage where there's increased resistance) [7-10]. The single greatest risk factor for type 2 diabetes in children is excess weight [11,12]. In Indian context, there are very limited literature and data paucity for implementation of new innovative and awareness programme for prevention of type-II diabetic in children [13,14].
In this context, the present study aims to know the prevalence of type II and their risk factors associated with different age group.
A retrospective observational sectional study was conducted at Department of Paediatrics, Bowring and Lady Curzon hospital, Bangalore during the period of 2015 - 2017. A total 450 children’s were screened in OPD and admitted ward. The demographic, risk factors, clinical factors, family history, type of food intake, duration of diabetes, type of previous medication, academic and physical exercise and other associated attributes were collected from the structured questionnaires. The inclusion and exclusion criteria rule was employed inclusion; cases age group 1 - 17 years irrespective age group and gender. Exclusion; HIV infected, terminal illness, intake of corticosteroids etc. Collected data were analysed by using Minitab. University analysis was employed to test the significant hypothesis.
The results (Figure 1) revealed that the prevalence of type II diabetes was seen more in male children as compared with female, there is no marginal difference between the occurrence of diseases at onset, the mean age of the cases was 11.25 ± 1.22 years in male cases and female was 12.85 ± 0.98 years (IQR 10 - 15 years). The overall prevalence was 9.65%. The major risk factors of type II diabetes were noticed during the study period, genetic complexity (p < 0.01), food intake high calorie(p < 0.01; odds 1.22), sedentary life-style (p < 0.01; odds 3.68), use of corticosteroids for healing wounds (p < 0.01; odds 4.01), lack of family support (p < 0.01; odds 2.58) are the pre-existing factors to derive the type II diabetes in child bearing age at an early stage. Elevated BMI (> 95th percentile), average 31.52 ± 1.22 kg/m2 is the deterministic factor to increase the incidence and prevalence of diabetes in children (P < 0.01, CI 95% 21.22 - 36.16 kg/m2), specificity 96.0%, sensitivity 78.0%, PPV 69%, NPV82%, AUC 0.89. A total 450 children were screened during the study period, the population was classified into two groups, the prevalence of diseases exposed population was 9.65% with greater accuracy 80.63%, good specificity 92.63% and sensitivity 86.56%. Net predicted value is apparently uncorrelated in unexposed population (p < 0.0001). Gender wise distribution of type-II diabetics in children was studied, as per the study the male was exposed more 13 (5.65%) when compared to female 8 (4.0%). The evidence was clearly illustrated that the inherited tendency is more common in male affected population.

Figure 1: Prevalence of type II diabetes status in males and females.
Prevalence of type-II diabetic in children’s different age group was represented in figure 2. The age groups were categorised based on mean age and their standard deviation. The present study four age groups were categorised, the age group between 1 - 4 years prevalence was (0.46%), none of the cases was found to be positive in females; 5 - 8 years (0.46%) males, females (0.52%); 9 - 13 years (2.76%) males and females was (1.56%) and similarly > 14 years was (2.30%) and female was (2.08%), in the overall population, the prevalence was (4.39%).

Figure 2: Prevalence of diabetes in different age group.
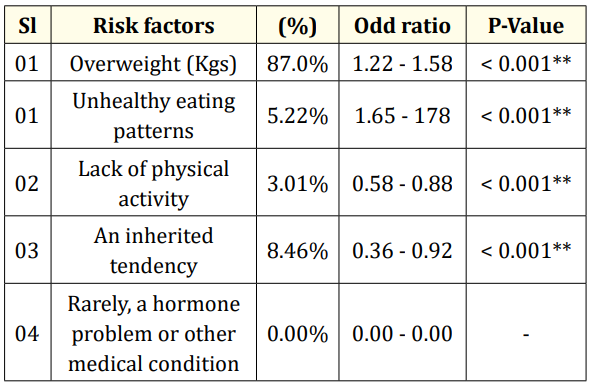
Table 1: Risk factors of type-II diabetics in exposed population.
The fewer number of information, paucity of literature about the epidemiological pattern of type II diabetes in Indian context among children is in the large part due to genetic complexity, lifestyle and food intake (high calorie food) another important factor is BMI > 95th percentile, cholesterol level > reference range, sedentary life life-style are the pre-exciting factors of type II diabetes. Sinha R., et al. [14], Krebs., et al. [3], Dietz., et al. [2] reported that, the obesity is a very common finding in children with type 2 diabetes [15]. In a young Pima Indian cohort reported that, with diabetes 85% were obese cases were seen highest risk of type II. This association deleteriously showed consistent results in all reports at global level. Although, the criteria for obesity and its severity have varied with individual age group. The study reported that, the mean BMI ranges from 27 - 38 kg/m2 and in most of the cases, since the BMI was found to be greater than the 85th percentile of mean age irrespective of sex. The resulted findings are being well established in adults and in many populations that a “Westernized lifestyle was greatly associated with an increased frequency of type II diabetes in children [2].
There are no well controlled studies that have examined this issue in children. Decreased exercise and increased calorie and fat intake have been implicated as risk factors [11]. Family history of diabetes is strongly associated with type II diabetes in children. The frequency of a history of type 2 diabetes in a first- or seconddegree relative has ranged from 74 to 100% [16]. Among Pima Indians below the age of 25 years, diabetes has been reported exclusively in individuals with at least one diabetic parent. In the Pimas, off springs of mothers who had diabetes during pregnancy had a markedly increased prevalence of diabetes as compared with off springs of normoglycemic mothers. As such being the case, the problem was continued to be replicated and described at population level, there remain a number of research needs. It will be necessary to better define the magnitude of type II diabetes in children and confirm that there is a significant difference trend toward the increasing incidence and prevalence. It will also be important to clearly define the characteristics of those affected has-been and the risk factors for developing the disease. Finally, it will be important to describe the natural history of the disease in those affected at young ages [2,3,14]. The recent increases observed in diabetes prevalence have occurred too quickly to be the result of increased gene frequency and altered genetic pool, emphasizing the importance of environmental factors. Increasing caloric expenditure by increasing daily physical activity is an important component of therapy. Exercise can decrease insulin resistance and is an important component of weight management. Decreasing sedentary activity, such as watching television and computer use, has been shown to be an effective way to increase daily physical activity in children. Involvement of family members can provide positive reinforcement and make overall family health a higher priority. Lack of physical activity is strongly associated with the development of obesity, type 2 diabetes and cardiovascular morbidity and mortality [17-19].
The present study concludes that, the type II diabetes is an alarming stage in Indian context due to sedentary life-style, separation of family, junk food intake and genetic complexity of the children etc. The resulted data are found to be narrowed; more number of studies would be needed for the policy intervention at population level. Encourage the children for practicing a good life-style and extrapolate the routine activities of children to support the positive guidance and healthy food choices to curb type II diabetes at an early stage. At the community level, schools, religious organizations, youth and family organizations and government agencies should assume to be endorse for wider scope and responsibilities for conducting Yoga and physical exercise regularly.
Copyright: © 2020 Basavarajaiah DM., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.