Valarmathi Selvaraj1*, Jain Vanitha2, Fabiola M Dhanraj3, Prema Sekar4 and Anitha Rajendra Babu5
1PhD (N) Scholar, Meenakshi Academy of Higher Education and Research, Virugambakkam, Chennai, India
2Professor, Director of Nursing Shenbaga College of Nursing, Chennai, India
3Principal, Arulmigu Meenakshi College of Nursing, Kancheepuram, India
4Principal, Annai Veilankanni College of Nursing, Perungalatur, India
5Principal, Rajalakshmi College of Nursing, Chennai, India
*Corresponding Author: Valarmathi Selvaraj, PhD (N) Scholar, Meenakshi Academy of Higher Education and Research, Virugambakkam, Chennai, India.
Received: March 06, 2020; Published: April 29, 2020
Citation: Valarmathi Selvaraj., et al. “Implementation of an Awareness Program and Lifestyle Intervention on Polycystic Ovarian Syndrome among Adolescent Schoolgirls in India”. Acta Scientific Paediatrics 3.5 (2020):24-30.
Authors share their experiences from a research on polycystic ovarian syndrome (PCOS) risk among adolescent schoolgirls in a South Indian state. One hundred and twenty school going adolescent girls from a government funded school in Southern India were assessed for PCOS risk, among which 40 had PCOS risk (moderate risk 36, high risk 4). These 40 were grouped in to either experimental or control which 20 each. Experimental group received awareness program and lifestyle modifications (yoga and exercise) by the researcher in coordination with the schoolteachers at the school premises. Pretest knowledge assessment showed, 16 (80%) in the experimental and 15 (75%) on the control group had ‘moderate’ knowledge. Post intervention, 15 (75%) had adequate knowledge in the experimental group and 9 (45%) in the control group. Knowledge score during pretest was mean 11.30; SD 4.91, t = 5.27; p = 0.000 in the experimental group, and 11.25; SD = 4.44, t = 2.85; p = 00.01 in the control group. Knowledge score of post-test was 11.30; SD 4.91; t = 5.27; p = 0.000 in the experimental and the mean 14.35; S.D 4.44; t = 2.85; p = 0.01 in the control group. Attitude score during pretest was 51.80; SD = 11.12, t = 0.01; p = 0.000 in the experimental and 53.45 SD = 5.91; t = 2.99; p = 00.01 in the control group. Attitude score during posttest was mean 53.45; SD = 5.91, t = 2.99; p = 0.1 in the experimental group and 53.45 SD = 5.91; t = 2.99; p = 00.01 in the control group. Improvements in knowledge and attitude score demonstrates the feasibility of lifestyle intervention targeted at adolescent girls, with PCOS risk, in school premises.
Keywords: Adolescent Girls; Attitude; Knowledge; Polycystic Ovarian Syndrome; Risk Assessment
PCOS is a hormonal disorder known to affect the females during their reproductive age (12 - 45 years). In India, it is considered as a growing problem with prevalence rate of among South Indian adolescent girls to be 9.13% [1]. PCOS is considered as metabolic and reproductive disorder characterized by excessive ovarian androgen production and chronic anovulation, which are responsible for irregular menstrual bleeding and hyperandrogens state (excessive male hormone) in adolescent girls [2]. As per the Rotterdam and Androgen Excess-PCOS Society criteria, there are three clinical phenotypes of PCOs (Frank PCOS, Ovulatory PCOS and Non-PCO PCOS (oligomenorrhea, hyperandrogenism, and normal ovaries). In addition, the Rotterdam criteria also recognize another type ‘Normoandrogenic PCOS’ [3]. In a study conducted among 100 women aged 15 - 25 years attending outpatient department in South India, 50 women had the history of irregular menstrual history and remaining 50 had regular menstrual history [4]. PCOS usually starts in adolescent stage and affect during childbearing age [5]. During adolescent stage, most of the cases are likely to be underdiagnosed [6]. It is diagnosed by the presence of 12 or more follicles in each ovary, increased ovarian volume (10 cm3) and measuring 2 - 9 mm in diameter [7]. Studies have investigated the effect of exercise on psychological outcomes in PCOS. A small, non-randomized study finding showed that overweight and obese women with PCOS reported that a six-month, self-directed brisk walking program improved body image distress. Yogic lifestyle modifications, a form of holistic mind-body medicine is a simple and easy to practice lifestyle process which is known to reduce anxiety symptoms related to PCOS [8-10].
There is an increasing number of adolescents presenting with signs of PCOS suggesting a higher possibility for cardiovascular, metabolic and depressive disorders [11-13]. Lifestyle modification such as yoga, exercise and diet help to reduce the risk of getting PCOS. Yogasana, commonly mentioned as ‘Yoga’ is a form of medicine developed thousands of years ago and has been popular in India for generations. It is simple and can be practiced by everyone and does not need much of infrastructure. Hence yoga is considered as a simple and easy means of exercise. Yoga helps to trigger the function of all endocrine glands and nerve plexus and help to maintain the hormonal level and to improve the fertility [14,15]. Risk assessment and lifestyle modifications appear to be the most useful strategy in approaching individuals at high risk for PCOS. India witnessed about 36% increase in PCOS cases in the last decade [8]. It is established that a small change in lifestyle are known decrease the symptom of PCOS. PCOS is a common problem among adolescent girls in India and early risk assessment and lifestyle interventions can be valuable alternative to treatment of the full-blown condition.
The aim of our study was to identify the PCOS risk among adolescent schoolgirls, to evaluate their knowledge and attitude towards PCOS, and to evaluate the effectiveness of awareness program aimed at improving knowledge, awareness and minimizing PCOS risks.
This research followed a quasi-experimental design in which the control group did not receive any intervention and experimental received intervention provided by the researcher.
In this present study, the population is school going adolescence girls who were studying in grades 10 - 12 at Government Girls Higher Secondary School, Kamaraj Nagar, Avadi, Chennai, South India. At the time of the research, the school had a total of 948 females.
The Ethical approval for the research was obtained from the Billroth Hospital Ethical Committee, Chennai, Tamilnadu State, India.
Since PCOS is common among adolescent girls and most of the adolescent girls attained their menarche before they studying 10th grades.
Participants who were adolescent girls who were studying in 10th to 12th grades, attained menarche for past 6 months during data collection, present at the time of data collection, who can read, speak and understand the local language (Tamil).
Adolescent girls who were not willing to participate in this research and perform lifestyle modifications, not attained menarche since attained menarche is the important in assessing the risk assessment, undergone educational program on PCOS through school education or in the community. Students who were routinely doing acrobatic exercise doing morning or evening, regularly doing Yoga in the morning or evening, sick on the time of data collection due to severe pain during menses, fever etc, and diagnosed as PCOS and taking medicine regularly, were also excluded.
This questionnaire was developed by the researcher. It has 25 multiple choice questions covering the anatomy of the reproductive system, definition, causes, signs and symptoms, diagnostic evaluation, complication and prevention of PCOS. A score of ‘1’ and ‘0’ was given to the correct and wrong answers respectively. The Cronbach ‘α’ value of knowledge tools was 0.84.
This questionnaire was developed by the researcher. It is a fivepoint Likert scale with minimum score ‘0’ and maximum score ‘4’. Scores were interpreted as ‘most favorable attitude’, ‘favorable attitude’ and ‘unfavorable attitude’. The Cronbach ‘α’ value of attitude tools was 0.86.
Simple random sampling technique was adopted by the investigator to select the samples. From 10th to 12th standards, the school had a total of 24 sections. In each of the sections the researcher selected 5 adolescent girls randomly and thus a total of 120 students were selected and the risk assessment questionnaire developed by Shoba., et al. [16] was administered. While analyzing the risk assessment questionnaire, it was is found that ‘high risk’, ‘moderate risk’, ‘low risk’ and ‘no risk’ students were 4, 36, 65 and 15 respectively. Among these 120 students, ‘high risk’ (n = 4) and ‘moderate risk’ (n = 36) adolescent girls were segregated and thus making a total of 40 students. These 40 adolescent girls were again randomly divided in to experimental and control group and the intervention are given by the researcher. After that pre-test on knowledge and attitude assessment was done by the researcher. The next day awareness program was given by the researcher. By the end of the seven days post-test on knowledge attitude assessment was performed by the researcher.
This session had 45 minutes Lecture with PowerPoint presentation given by the Researcher about, definition, causes, pathophysiology, complication, and prevention of PCOS.
During this session, Yogasana was given by the researcher 30 minutes daily morning for 3 days. The Yogasanas included Pranayama, Bhadrasana, Chakki Chalanasana, Bharadvajasana and Sun salutation.
Three days brisk walking exercises given by the researchers for 30 minutes.
All the above three sessions were conducted in coordination with the schoolteachers at the school.
The filled knowledge and Attitude questionnaires were entered in to the SPSS and demographic variables, risk assessment, knowledge and attitude questionnaire were analyzed. The pretest and posttest knowledge score and attitude score were confirmed by’ ‘independent t test’.
In the experimental group 12 (60%) of the girls age is 16 and 20 (100%) of the girls attained age of menarche in 11 - 14 yrs. Further details regarding the demographic details of the study subjects are tabulated in table 1.
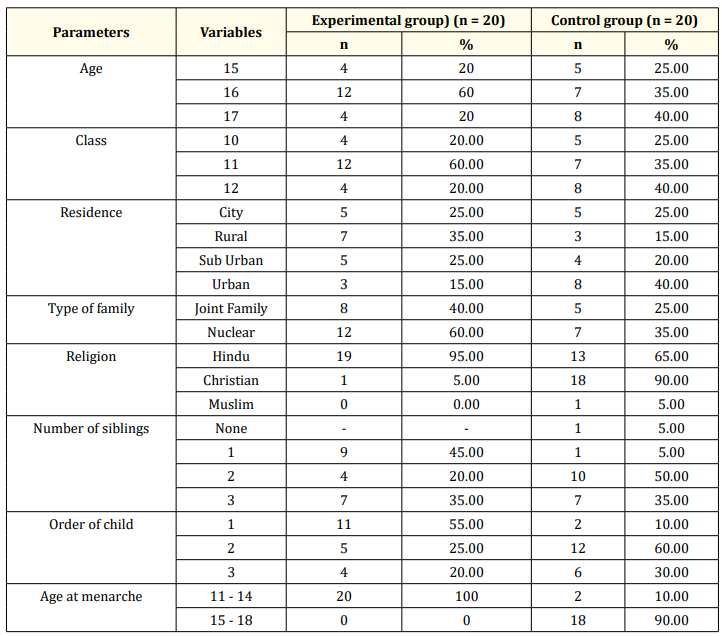
Table 1: Demographic characteristics of the respondents (n = 40).
Majority of the fathers in experimental group was daily wages and none of the respondent family income is more than Rs. 7000 (USD = approximately 70.00 INR). Among control groups, most of the parents were daily wages and semiskilled 6 (30%) and only 4 (20%) of the respondents’ family income is more than 7000. Further details regarding the demographic details of the study subjects are tabulated in above table 2.

Table 2: Demographic characteristics of respondents’ parents.
Note: The total numbers may not match as few of the respondents might have not filled certain responses.
Sources of information relied by the respondents: Table 3 Shows the frequency and percentage of the sources of information relied by the respondents in relation to health information.
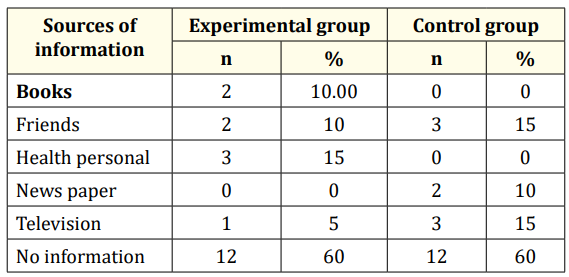
Table 3: Frequency and percentage of the sources of information relied by the respondents.
Table 4 shows that the comparison of the total scores of height, weight and body mass index was found to be 157.11, 47.30, 20.31 in experimental group and 153.30, 47.30, 0.11 in control group respectively.
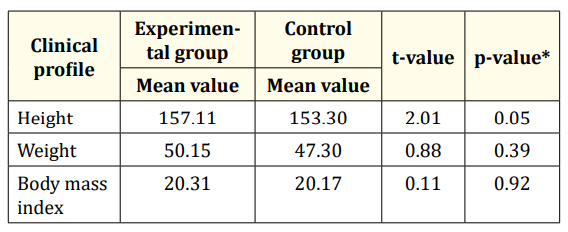
Table 4: Comparison of the total scores of clinical profile of risk girls (experimental group and control group). P value of < 0.05 was taken as statistically significant. *= independent ‘s’ test.
Impact of intervention on risk scores: In the experimental group, most of the respondents 19 (95%) were having moderate risk and only 1 (5%) were having high risk. In control group all the respondents were having moderate risk and none of them were had high risk. In posttest experimental group 18 (90%) were having moderate risk and only 2 (10%) were having high risk (Table 5).

Table 5: Pretest and posttest frequency and percentage of risk assessment.
Table 6 shows the frequency and percentage of pretest level of knowledge in experimental and control group. In pretest experimental group majority of the respondents 16 (80%) were having moderate knowledge. Remaining 3 (15%) were having in adequate knowledge and only 1 (5%) respondents having adequate knowledge. In control group majority of the respondents were 15 (75%) having moderate knowledge.

Table 6: Knowledge score evaluation.
Table 7 shows the impact assessment of intervention on knowledge scores among both the groups.

Table 7: Impact assessment of intervention on knowledge scores. P value of < 0.05 was taken as statistically significant. *= Independent ‘t’ test.
Table 8 shows the difference in the pretest and posttest attitude in experimental group confirmed by the independent ‘t’ test (2.83), which was significant at p < 0.001. The difference in the pretest and post test scores of the attitude in control group confirmed by the independent ‘t’ test (2.99), which was significant at p < 0.001.

Table 8: Attitude assessments. P value of < 0.05 was taken as statistically significant. *= Independent ‘t’ test.
Uncontrolled PCOS is associated with pregnancy-induced hypertension, preeclampsia, gestational diabetes mellitus, hypertension, dyslipidemia, type-2 diabetes mellitus, mood disorders, and can lead to increased cancer risks [17]. This research identified beneficial effects of lifestyle modifications on PCOS risk among adolescent girls and in addition showed positive impact on their knowledge and attitude towards PCOS. It is well known that exercise helps to improves autonomic function and inflammatory pattern in women with PCOS. In this study, the experimental group students had a better improvement in their PCOS risk reduction. Since their knowledge and attitude also increased, this positive outcome may provide a sustainable reduction in further PCOS risk.
Health education is crucial since it largely influence the manner which it is responded. Often mothers are the source of health education on early symptoms identification and eating habits of their daughters. A similar study conducted at Egypt [18] showed that that only a few mothers were graduates. A mother’s response to health problem of the child is deemed crucial [19,20]. Family income may be considered as a predictor for PCOS risk as it is linked with eating junk foods. However, in studies from India [16] and Saudi, the level of monthly income did not have any influence PCOS knowledge [21].
In the present study most of the participants did not had any information on PCOS and their dependence on resources such as newspapers, television, etc were minimal. However, few of them had received minimum info only from friends, health personnel and books. These findings were associated with a study in which 80 (100)% had no information about PCOS [22]. Another study showed that 19% had information from their friends, 3.5% from newspaper and 28% were unaware about PCOS [23]. The intervention in the current research is targeted at motivating students to learn more about PCOS through all available resources.
Most of the respondents had moderate risk and only very few had high risk. In one study, authors found menstrual cycle disorder, bad mood, family history of diabetes, and family history of infertility menstrual irregularity of mother and lack of physical exercise as risk factors for PCOS [24]. This research did not focus much on PCOS risk reduction as it was conducted only for a short period. Long term studies will be valuable in identifying impact of such interventions on PCOS risk reduction.
During pre-test phase of the current research, majority of the girls had inadequate knowledge, which upon intervention turned much better post intervention. A study from Egypt assessed the impact of an educational program on PCOS among adolescent girls and researchers found enhancement of knowledge scores which was poor in case of 84% of the students prior to the intervention [15]. It is important to have a sustainable improvement in knowledge scores as it can potentially improve the attitude and practice towards PCOS. In this research efforts have been put to improve various aspects of knowledge such as pathophysiology, symptoms, causes of PCOS etc.
During pre-test majority of them had unfavourable attitude towards PCOS. After intervention, majority of them had favourable attitude. One study from The Netherlands evaluated the relationship between PCOS characteristics and psychological wellbeing. The results revealed notable impairment of psychological wellbeing of the individuals with PCOS symptoms [25]. Hence it is important for any interventions should focus on improving the psychological features of the individuals with PCOS. There is a possibility that the respondents between the control and experimental groups interacted and discussed on the topics related to PCOS and thus making it a potential limitation of this research.
The findings of this research show the improvement in knowledge and attitude scores upon educational intervention. Thus, it is feasible to incorporate an education module for school going adolescent girls at risk for PCOS and helping in early identification and prevention of the illness.
Authors acknowledge all the students who actively participated in this research. Special thanks to the schoolteachers and School administration for their participation and granting permission.
Nil.
None.
Copyright: © 2020 Valarmathi Selvaraj., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.