Rafik Shalaby1 and Mohamed Ahmed Negm2
1Department of Pediatric Surgery, Al-Azhar University, Cairo, Egypt
2Pediatric Surgery Unit, Qena Faculty of Medicine, South Valley University, Qena, Egypt
*Corresponding Author: Mohamed Ahmed Negm, M.D, Pediatric Surgery Unit, Qena Faculty of Medicine, South Valley University, Qena, Egypt. E-mail: drmohamednegm@yahoo.com Official E-mail : drmohamednegm@med.svu.edu.eg
Received: January 17, 2020; Published: January 29, 2020
Citation: Rafik Shalaby and Mohamed A. Negm. “Laparoscopic Snaring of Hernia Sac for Inguinal Hernia in Girls: A Preliminary Study”. Acta Scientific Paediatrics 3.2 (2020):48-52.
Background: Although open inguinal herniotomy is considered the gold standard for inguinal hernia in all pediatric ages, recently laparoscopic repair with different techniques gained popularity and became widely practiced in many centres worldwide and became one of alternative option for inguinal hernia repair in infant and children. This study reported the initial experience of a novel technique of laparoscopic inversion and snaring of inguinal hernial sac with peritoneal closure of defect at the internal inguinal ring [IIR] in girls.
Methods: Thirty-seven girls with inguinal hernia were subjected to laparoscopic inversion, snaring herniotomy with peritoneal closure at IIR. Follow-up period were more than 10 months.
Results: Thirty-seven girls with 55 hernias were included. Mean age was (39.8 ± 18.1 SD) months. Eighteen (48.64%) girls presented with right sided, 8 (21.62%) girls with left sided, and 11 (29.72%) girls were bilateral CIH Intraoperatively, 7 of U/S diagnosed unilateral cases were found to have a contralateral hernia. In 5 (13.5%) patients associated umbilical hernia were present that repaired in the same sitting. There were no perioperative complications and all cases were completed successfully without conversion. The mean operative time in minutes was (19.5 ± 3.1 SD) in bilateral while it was (12.4 ± 1.6 SD) in unilateral cases. Follow up period was ranged from 10 – 33 (Mean 25.02 ± 6.67 SD) months with no detected recurrence among the studied patients.
Conclusion: Laparoscopic inversion and snaring of the hernia sac with closure of the peritoneal defect is a safe, rapid and feasible method for inguinal hernia repair in girls without recurrence.
Keywords: Inversion; Hernia sac; Laparoscopy; Girls; Closure of the Peritoneal Defect; Snaring
IIR: internal inguinal ring; CIH: congenital inguinal hernia
For the pediatric surgeon, inguinal hernia repair is the frequently surgical operation in daily practice [1]. Although open surgery is considered the gold standard for all pediatric ages, recently laparoscopic repair gained popularity and became widely practiced in many centres worldwide [2, 3] and became one of alternative option of inguinal hernia repair [4].
Laparoscopy for inguinal hernia was firstly done in girls by El Gohary in1997 [5], since then many laparoscopic techniques for inguinal hernia repair was developed aiming for achieving the advantage of minimal invasive surgery and decreasing the rate of recurrence [6-8].
It is well known that, inguinal hernia repair by laparoscopy in girls is a good candidate for improvement and upgrading the learning curve of laparoscopic skills of young surgeon. According to our best knowledge in the English literature there is no reported data about laparoscopic inversion and snaring of inguinal hernial sac at IIR with peritoneal closure of defect in girls. The goal of this study was to present the preliminary experience of this new technique. We refer to this technique as laparoscopic inversion, snaring of hernia sac and peritoneal defect closure in girls.
Over a period of 36 months from the 1st of January 2016 to the 1st of January 2019 a prospective two centres study included 37 girls presented with inguinal hernias. After ethical committee agreement, we included in this study only female children presented by inguinal hernia of one or both sides. Recurrent hernia, complicated cases and cases with internal ring diameter more than 15mm measured by preoperative U/S were excluded. Preoperative routine laboratory investigation and inguinal ultrasound to assess the presence of other side and measuring the diameter of both IIR was done.
All patients were repaired using laparoscopic inversion and snaring of the hernia sac with peritoneal closure.
Under general anesthesia with Trendelenburg position, initial assessment of both internal rings. The diameter of open internal ring was measured as proposed by Shehata., et al. [9].
Laparoscopic hernia sac inversion was done as described by Lipskar., et al. [10] where hernia sac was completely inverted into the peritoneal cavity. This accomplished through insertion of the ipsilateral Grasper into the hernia sac to grasp its fundus. With freeing any adhesions around the sac, it was twisted on itself 2-3 times. Then the contralateral trocar was removed.
The snare demonstrated in figure 1 was introduced into the abdominal cavity along the 3 mm grasper from the site of removed trocar. The ipsilateral Grasper was passed into the snare and the hernia sac was re-grasped again and twisted as shown in figure 2 so, the inverted, twisted hernia sac was snared and cauterized slowly with low monopolar cutting diathermy at the neck in interrupted manner.
![Figure 1: The Snare, [A-Loop of the Snare opened, B-Loop of
the Snare closed] “Acusnare polypectomy snare [Cook Medical,
Wilson-cook Medical, Inc.4900 Bethania Road Winston-salem
NC27105. WWW. Cookmedical. com].](https://actascientific.com/ASPE/images/IJMCR/ASPE-03-0210-fig1.PNG)
Figure 1: The Snare, [A-Loop of the Snare opened, B-Loop of the Snare closed] “Acusnare polypectomy snare [Cook Medical, Wilson-cook Medical, Inc.4900 Bethania Road Winston-salem NC27105. WWW. Cookmedical. com].
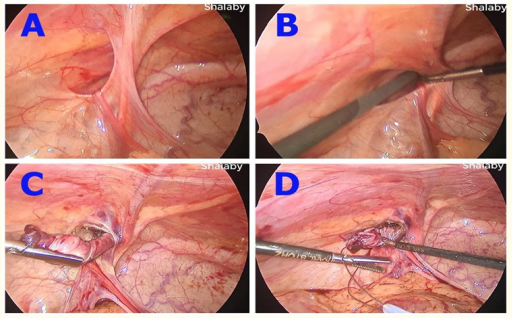
Figure 2: Steps of inversion and insertion of the snare.
A. Left inguinal hernia in a girl.
B. The ipsilateral Grasper is inserted into the hernia
sac to grasp its fundus.
C. Inversion and twisting the hernia sac.
D. The Grasper is passing into the opened snare loop.
The twisted snared distal sac was extracted and peritoneal defect was closed with polypropylene suture as shown in figure 3. In bilateral, cases the same technique was repeated. The umbilical incision was closed after umbilical herniotomy if present. This video link for more details about laparoscopic inversion, snaring and peritoneal closure technique: https://drive.google.com/open ?id=1lU9c8VHH0VQZRxUe1G3W8FmFkYvYGtAf.
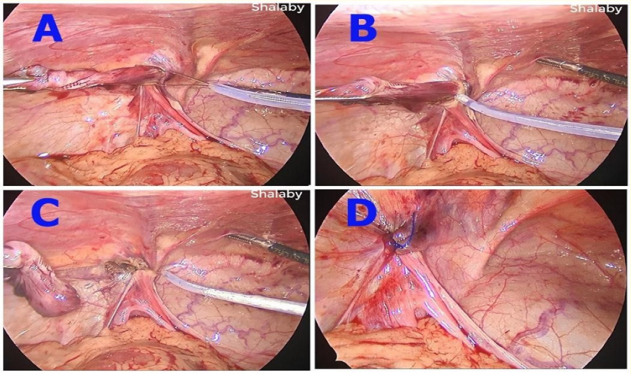
Figure 3: Steps of snaring and suturing of small peritoneal
defect.
A. Opened loop of the Snare is encircling the twisted invert
ed sac snugly and precisely
B. Closed loop of Snare around the twisted inverted with
generation of a low current cutting mode diathermy and
proceeding carefully with short buzzes
C. Complete division of the sac with narrow raw area at its
neck without much diathermy to the surrounding sutures
D. Closure of the narrow raw area of peritoneal defect
Follow-up was done in out-patient clinic weekly for 2 weeks for the first month, then every 3 months in the first year. All parents were instructed to attend if any abnormality was appeared specially groin swelling.
This study was carried out on 37 girls with 55 inguinal hernias as shown in figure 4. Five (13.51%) patients had associated with umbilical hernia. The patient’s age, operative time and follow up period are shown in table 1. All hernia repaired by laparoscopy using the same technique principles of inversion, snaring of hernia sac with peritoneal closure. No conversions to other laparoscopic techniques or open method were needed in this study. Although the technique was easy and take short time, there were some difficulties in complete inversion the hernia sacs especially in early cases. But after getting familiar with the technique, it became easily done in a shorter time. All patients were discharged from the hospital in the same day. There were no perioperative complications. Associated umbilical hernias were simultaneously repaired in the same setting with no detected complication. The mean follow up was (25.02 ± 6.67 SD) months with no recurrence detected among the studied patients.
![Figure 4: Number of patients and hernias.
[* These cases were found to be bilateral].](https://actascientific.com/ASPE/images/IJMCR/ASPE-03-0210-fig4.PNG)
Figure 4: Number of patients and hernias. [* These cases were found to be bilateral].
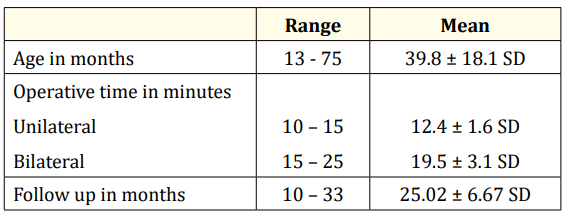
Table 1: Study demographic data.
Over the past years, laparoscopic hernia repair became a wellestablished and popular technique for inguinal hernia in children with good cosmetic outcome in comparison to the standard open technique and the recurrence after surgery. Moreover, laparoscopy allows diagnosis of contralateral hernia can be achieved with simultaneous repair [4,11-13]. The only drawback of this technique is the need of long learning curve compared by conventional open surgery [14].
Laparoscopy for inguinal hernia repair by inversion and ligation using endo loop was first introduced by El Gohary in 1997. This operation initially carried out in females because it is safer than males due to absence of vas and testicular vessels [5].
Another study by Felix Schier in 1998 and included 14 girls repaired by intracorporeal suture for closing the internal ring by two or three Z suture [15].
Recently, there are many other techniques available for application of laparoscope in inguinal hernia repair especially in girls as inversion ligation, inversion with cauterization and percutaneous ligation [6-8,16-18].
The technique of snaring discussed in this study is used in polypectomy in colonic polyps by the technique of cold or hot snaring with excision of polyps without colonic wall perforation [19].
In the present study, the snare was attached to low current cutting diathermy to decease spread of heat to surrounding structure. We proposed that inversion, encirclement and snaring of the hernia sac results in a herniotomy with narrow raw area at its neck. Moreover, combining herniotomy with peritoneal closure result in sound healing that may prevent or minimize recurrence.
Blatnik., et al. demonstrated experimentally in rabbit models that, intentional peritoneal injury at the site of closure produce durable repair [20] In a study by Novotny., et al. they used the Maryland for inversion and cauterization of the hernia sac in 67 girls with 80 hernias, they added that no recurrence were developed on 25 months follow up only one case complicated by hernia but at the site of side trocar [21] St-Louis., et al. in their study of the effect of thermal injury on the hernia sac using monopolar cautery applied on the anterolateral aspect of the internal ring in 94 female and 178 male children, they reported 3% recurrence rate. They also concluded that ―intentional peritoneal thermal injury was not associated with recurrent rate improvement in their study‖. This may be due to application of thermal cautery of diathermy without excision of hernia sac [22].
In a recent study by Marte., et al. on 28 children of them 12 were girls. They utilized simple internal ring cauterization as done in Burnia technique of Novotny., et al. [21] through transumbilical trocar using a grasper; the sac was inverted and wrapped the grasper in a spaghetti manner. Application of monopolar coagulation diathermy to the grasper itself, the hernia sac will be shrunken with closure of internal ring.
No recurrence was reported with any perioperative complication except for lymphocele developed at the level of labium major in a 6 years girl 2 weeks postoperatively with improvement after 6 months [23].
According to the result of this study, the advantages of inversion, snaring and peritoneal closure technique are short operative time and adequately remove the whole sac in one mass with no remaining peritoneal bridge that may be the cause of recurrence. No recurrence also reported by Zallen and Glick in their study using laparoscopic inversion, twisting and ligation by monofilament absorbable endoloop [6]. Guner., et al. using the same technique with very good result except 2 patients presented by recurrence due to non-excised sac. In the same conversion to open technique was required in another two patients with sliding type hernia [7]. We agreed with other authors that girls are good candidate for applying new innovative laparoscopic hernia repair techniques because there is no vas and vessels passing through the IIR. In addition, the majority of young laparoscopic surgeon and resident usually start their training curve with inguinal hernia repair in girls [8].
In this study, this novel technique laparoscopic inversion, snaring of hernia sac and peritoneal closure enables to perform laparoscopic hernia repair in girls easily and efficiently with short time of surgery when compared to others [7]. In the current study, there is no reported recurrence, this may attributed to sac excision together with peritoneal closure by nonabsorbable suture as reported by others [24]. Although this a preliminary study, the results are encouraging to draw a definite conclusion.
The small number of cases together with inclusion of female children only but, this a preliminary study with further studies specially randomised controlled trials are needed. Another limitation of this study was the price of disposable snare but, its value in decreasing the operative time together with the simplicity of the technique overcome addition of its high price.
Laparoscopic inversion and snaring of the hernia sac with peritoneal defect closure is reproducible easy and promising method for inguinal hernia repair in girls. It resulted in marked reduction of operative time without recurrence however; further studies and randomised trials are needed.
None.
None.
Copyright: © 2020 Rafik Shalaby and Mohamed A. Negm. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.