Shafi Ahmed1*, Swapan Kumar Chowdhury2, Muhammad Mozammel Haque3, Palash Chandra Banik4, Rabeya Yasmin5, MH Faruquee6, SK Akhtar Ahmad7 and AFM Salim8
1Associate Professor, Department of Pediatrics, Khwaja Yunus Ali Medical College and
Hospital, Shirajganj, Bangladesh
2PhD Fellow, Bangladesh University of Professionals, Bangladesh
3Consultant Pediatrics, Mahbubur Rahman Memorial Hospital and Nursing Institute,
Rupashdi, Banchharampur, Brahmanbaria, Bangladesh
4Assistant Professor, Department of Non-communicable Diseases, Bangladesh University of Health Sciences, Bangladesh
5Assistant Professor, Department of Occupational and Environmental Health,
Bangladesh University of Health Sciences, Bangladesh
6Associate Professor, Department of Occupational and Environmental Health,
Bangladesh University of Health Sciences, Bangladesh
7Professor, Department of Occupational and Environmental Health, Bangladesh
University of Health Sciences, Bangladesh
8Ex-Professor, Institute of Child Health and Shishu Swasthya Foundation Hospital,
Mirpur, Dhaka, Bangladesh
*Corresponding Author: Shafi Ahmed, Associate Professor, Department of Pediatrics, Khwaja Yunus Ali Medical College and Hospital, Shirajganj, Bangladesh.
Received: January 02, 2020; Published: January 10, 2020
Citation: Shafi Ahmed., et al. “Growing Pain Among Bangladeshi Children: Urban and Rural Settings”. Acta Scientific Paediatrics 3.2 (2020):21-25.
Vitamin D plays role in regulating cell growth, maintenance of body immunity, healthy musculoskeletal structure and functioning other various biological activities in keeping people healthy. This study was a part of a community based cross sectional study which was conducted among 274 primary school children. Two primary schools were selected purposively (one from Dhaka city and one from Gazipur district). The male and female ratio was equal. The mean age of the students was 8.86 ± 2.035 years. Majority of the children were within 5 – 10 years (73.7%) and rest were within 10 – 14 years. The male and female ratio was equal. Among the participants 28.8% were in class I, 20.1% were in class II, and 16.4% were in class III, 17.9% in class IV and rest 16.8% were in class V. Among the study participants 48.2% were of rural areas and 51.8% were from urban area. Among the participants, 97.0% of the rural areas and 75.4% of the urban areas had growing pain. By pain status of the rural participants, 89.8% reported their pain as mild and 10.2% as moderate while 38.3% of urban participants reported their pain as mild, 60.7% as moderate and 0.9% as severe. Statically significance association was found between residence of the participants with development of growing pain and increasing manner of pain status (p< 0.05). Among the rural children 60.9% had no scope of regular sun exposure, while among the urban children it is 27.1% (p< 0.05). Growing pain was reported in increasing manner among those who had scope of sun exposure for 2 hours per day, for 2 – 5 hours and who had no scope of regular sun exposure (p< 0.05). Prevalence of growing pain and insufficient sun exposure especially among rural school going children in Bangladesh is very high and alarming which needs to explore the root cause.
Keywords: Growing Pain; Children; Urban and Rural Settings; Bangladesh
Musculoskeletal pains are the common phenomenon of Growing pains, or recurrent lower limb pains, among 49.4% of children worldwide. The growing pains are found prevailing globally among 3 to 37% children [1,2].
The clinical features of Growing pains are cramping or achy muscle pains [usually in late afternoon or evenings] in both legs that some preschool children often complain. Sometimes children may waken in the middle of the night due to these pains. Growing pains generally observed to be started in early childhood, within the age of 3 or 4 years and also may attack back within the age of 8-12 years of the victims [3,4]. This pain is generally non-articular, intermittent, bilateral type and not limiting children’s mobility [5,6]. Exercise may aggravate the pain and which may last for few minutes to hours. No sign of inflammation on physical examination and laboratory investigation generally detected [7]. Growing pains are generally non-progressive towards any organic disease and usually resolve by adolescence period [8].
Holick mentioned in his articles that deficiency of Vitamin D might be the causes of muscular weakness and muscle pain among children and adults as well [9,10]. Unfortunately, one child cannot receive enough vitamin D from dietary sources alone. Instead, like adults, children must rely on sunshine and supplements to maintain healthy vitamin D levels [11]. In human body, around ninety percent vitamin D generally derived from sunlight and rest from dietetic intake. Both physical and environmental factors may affect individual’s exposure to sunlight and thus limit the ability of production of vitamin D endogenously within their body [12]. Deficiency of Vitamin D is now a day’s been identified as the evidence of lifestyle disorder in the urban population even after abundant sunlight. They are fail to expose themselves to sunlight due to long school time, lack of physical activities and exercises [13].
This study is an attempt to find out whether there is any association between sunlight exposure and development of growing pain among Bangladeshi children.
This study was a part of a community based cross sectional study which was conducted among 274 primary school children during July 2018 to June 2011. Two primary schools were selected purposively (one from Dhaka city and one from Gazipur district). After taking written informed consent from guardians all required data were collected. Socio-demographic information including age, household size, education of parents or caregiver, income, employment of the head of the households and housing condition were recorded.
Site, time and frequency of pain were obtained along with family history of similar pain and the pain relieving methods using questionnaire. Pain severity was evaluated using Visual Analog Scale{VAS}, a linear scale where a score from 0 to 10 is marked according to the severity of pain. Children were asked to mark the severity of pain they experienced during the last attack.
Sun exposure history was taken by interview whether the study participants stay outside especially when the sunlight is maximum (generally 10 am. to 4 pm). Participants also been asked to record their primary activities during this specific time. Physical activity was evaluated using questionnaire regarding type, frequency, and duration of each exercise. Sun exposure was assessed using questionnaire regarding the duration of exposure.
Among the study participants, male female ratio was equal. The mean age of the study subjects were 8.86 ± 2.035 years. Majority of the children were within 5 – 10 years (73.7%) and rest were within 10 – 14 years. The male and female ratio was equal. Among the participants 28.8% were in class I, 20.1% were in class II, and 16.4% were in class III, 17.9% in class IV and rest 16.8% were in class V. Around 48% study participants were of rural areas.
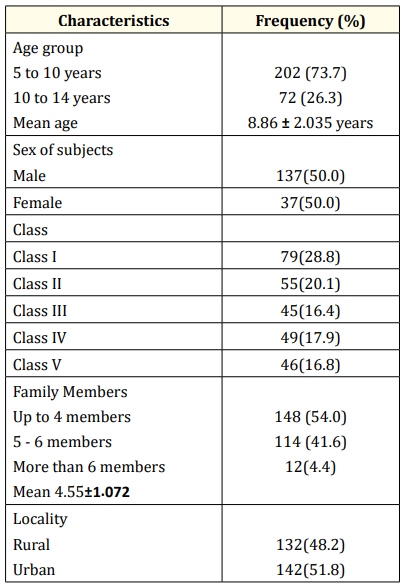
Table 1: Socio-demographic distribution of subjects (n=274).
Among the mothers of the subjects, 76.3% were housewife while rest were found engaged with individual profession. Among the fathers 26.3% were service holder, 16.8% were engaged with business and rest were found engaged in different profession. The education level of the mothers were found as 16.4% had no institutional education, 44.9% had primary level, 31.4% had secondary level (up to SSC), 4.7% had up to HSC level and 2.6% were graduate. That of father was found as 14.2% had no institutional education, 38.0% had primary level, 37.6% had secondary level (up to SSC), 5.5% had up to HSC level and 4.7% were graduate.
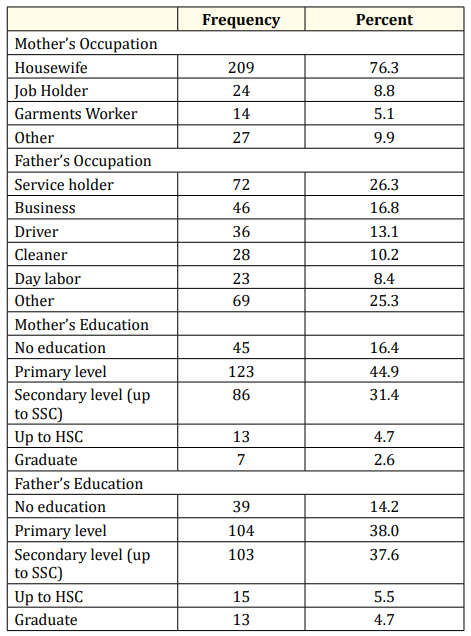
Table 2: Distribution of respondents by socio-demographic characteristics.
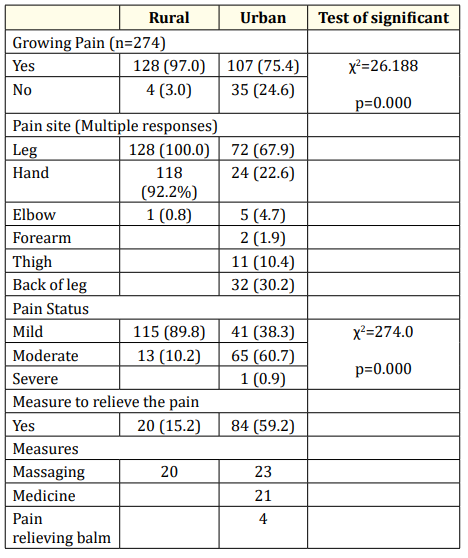
Table 3: Growing pain status of school going children: Rural-Urban Settings.
The table 3 shows that 97.0% of the rural participants and 75.4% of the urban participants had growing pain. Of the rural participants who had growing pain, every one complaints of pain in leg, 92.2% in hand, while among those of urban participants, 67.9% complaints of pain in leg followed by 22.6% in hand, 10.4% in thigh and 30.2% in back of leg. By pain status of the rural participants, 89.8% reported their pain as mild and 10.2% as moderate while 38.3% of urban participants reported their pain as mild, 60.7% as moderate and 0.9% as severe. Among the rural participants 15.2% mentioned that they practiced massaging to get relief of pain while among the urban participants 59.2% one fourth practiced massaging and another fourth took medicine and pain relieving balm. Statically significance association was found between residence of the participants with development of growing pain and increasing manner of pain status (p< 0.05).
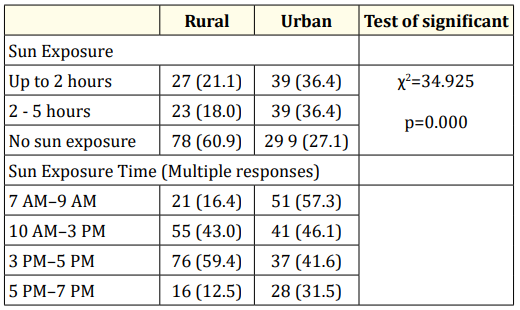
Table 4: Sun Exposure of school going children: Rural-Urban Settings.
Table 4 is describing that among the rural children 21.1% were accustomed to sun exposure for 2 hours per day, 18.0% for 2 – 5 hours per day and 60.9% had no scope of regular sun exposure. On the other hand among the urban children, 36.4% were accustomed to sun exposure for 2 hours per day, 36.4% for 2 – 5 hours per day and only 27.1% had no scope of regular sun exposure. Statistically it was found highly significant (p<0.05).
By timing of sun exposure it was reported that rural children had the scope of sun exposure during 7 AM–9 AM by 16.4%, 10 AM–3 PM by 43.0%, 3 PM–5 PM by 59.4% and during 5 PM–7 PM by 12.5%. Urban children had the scope of sun exposure during 7 AM–9 AM by 57.3%, 10 AM–3 PM by 46.1%, 3 PM–5 PM by 41.6% and during 5 PM–7 PM by 31.5%.
Growing pain was reported in increasing manner among those who had scope of sun exposure for 2 hours per day (86.8%), who had scope of sun exposure for 2 – 5 hours per day (73.8%) and who had had no scope of regular sun exposure (93.9%). Statistically it was found highly significant (p<0.05).
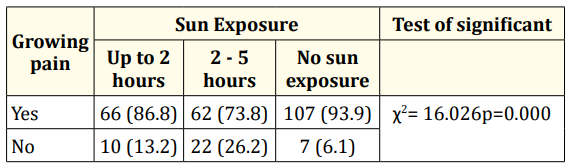
Table 5: Association between developing of growing pain and sun exposure among the participants.
The study was conducted among the primary school students of rural and urban settings. This current study included a total 274 children of whom 132 were from rural area and 142 were from urban area with equal male female ratio. Among the subjects, seventy four percent were in the age group of 5 to 10 years age followed by twenty six percent were in the age group of 10 to 14 years of age with mean 8.86 ± 2.035 years. Among the mothers of the subjects, seventy six percent were housewife while rest were found engaged with individual profession. Among the fathers more than one-fourth were service holder, seventeen percent were engaged with business and rest were found engaged in different profession. The education level of the mothers, around sixteen percent had no institutional education, forty five percent had primary level, and thirty one percent had secondary level (up to SSC) of education. And that among the father, fourteen percent had no institutional education, thirty eight percent had primary level, around same percent had secondary level (up to SSC) education.
This study revealed that 97.0% of the rural participants and 75.4% of the urban participants had growing pain. The most common sites of growing pain was leg followed by in hand. By pain status, among the rural participants, 89.8% reported their pain as mild and 10.2% as moderate while among the urban participants 38.3% reported their pain as mild, 60.7% as moderate and 0.9% as severe. Among the rural participants 15.2% mentioned that they practiced massaging to get relief of pain while among the urban participants 59.2% either practiced massaging or medicine and pain relieving balm.
Growing pain was reported in increasing manner among those who had scope of sun exposure for 2 hours per day, for 2 – 5 hours per day and who had had no scope of regular sun exposure.
There is no general guidelines on the amount of sun exposure needed to maintain adequate vitamin D levels in body. But adequate sun exposure between 10 AM and 3 PM to the face, arms, legs, or back without sunscreen is suggested by some scientists for sufficient vitamin D synthesis. This study interestingly found that a major portion of rural children (60.9%) had no scope of regular sun exposure which was 27.1% among urban children. Sun exposure during 3 PM–5 PM was reported by 43.0%, rural and 43.0% urban children. Studies conducted in Jeddah, Saudi Arabia [14] and Malaysia [15] found that due to hot and humid weather school going children have to stay indoor most of the time and loss scope of adequate sun exposure. Increasing internet based recreation may be one cause of less sun exposure by school going children in Bangladesh instead of physical exercise and playing in open ground field.
The prevalence of growing pain and insufficient exposure to sunlight especially among rural school going children in Bangladesh is very high and alarming which needs to explore the root cause. Promotion of healthier lifestyle involving regular outdoor physical activity may improve the situation.
The teachers and guardians of the participants are also highly acknowledged
Authors declare that they have no conflict of interest.
Copyright: © 2020 Shafi Ahmed., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.