Lise-Lotte Larsson1, Irini Antoniadou2, Gunilla Björling3 and Janet Mattsson4*
1 Perioperative Medicine and Intensive Care, University Hospital, Stockholm, Sweden
2 The Swedish Red Cross University College, Department of Health Sciences, KTH Royal Institute of Technology, School of Engineering Sciences in Chemistry, Biotechnology and Health, Department of Biomedical Engineering and Health Systems, Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, Sweden
3 The Swedish Red Cross University College, Department of Health Sciences, Karolinska Institute, Department of Neurobiology, Care Sciences and Society, Stockholm, Sweden
4 The Swedish Red Cross University College, Department of Health Sciences, Department of Learning, Informatics, Management and Ethics, LIME, Karolinska Institute, Sweden
*Corresponding Author: Janet Mattsson, The Swedish Red Cross University College, Department of Health Sciences, Department of Learning, Informatics, Management and Ethics, LIME, Karolinska Institute, Sweden.
Received: November 18, 2019; Published: November 28, 2019
Citation: Janet Mattsson., et al. “Healthcare Professionals Use of Mobile Phones in the Operating Theatre”. Acta Scientific Paediatrics 2.12 (2019): 66-72.
Background: Today mobil phones has been incorporated in our daily lives to such an extent that they are used in the operating theater for both professional and private matters. The advantages and disadvantages associated with the use of mobile phones in the healthcare sector are described in studies.
Aim: To describe healthcare professionals use and managing of professional phones and private mobile phones in the operating theater
Method: The design is a descriptive cross-sectional study with 40 structured observations in the operating theater and a questionnaire survey. The study was conducted in three surgical departments at a Swedish children's hospital. The participants were anesthetic nurses, physicians, operating theater nurses and assistant nurses. Data was analyzed descriptively in SPSS.
Result: The observations showed that of 477 phone uses, 287 (60.2%) were private mobile phones and 190 (39.8%)professional phones. The adherence to basal hygiene guidelines before and after telephone use, n = 477, was 93 (19.4%) and 103 (21.5%), respectively. The questionnaire showed that 9 (27.2%) of the participants experienced daily that the use of private mobile phones disturbed team members in the operating theater. Eight (24, 2%) of participants experienced daily, 7 (21.7%) weekly, employees became less concentrated due to the use of private mobile phones.
Conclusion: Increased compliance with basic hand hygiene guidelines, designing policies regarding the use of private mobile phones in the operating theater and a discussion concerning what is ethically correct in relation to the patients can be considered essential. Further studies are needed for continued exploration of the use and managing of mobile phones in the operating theater.
Keywords: Healthcare; Operating Rooms; Mobile Phones
Mobile phones are a normal companion in our everyday life. They are taken for granted to an extent that it is common that healthcare professionals use mobile phones for both professional and personal issues in the workplace [2,5,20,28,29] and younger employees tend to use private cell phones more often than older [7,17,19,20]. It has been reported that more than 78 percent of healthcare professionals use their private mobile phones at work [3,5,7,17,20,25,32]. However, the healthcare professionals find it difficult to draw the line between using private mobile phones for professional and private use, as they find it difficult to ignore private calls and messages [20]. There is however very little research about the patient safety and ethical implications of mobile phone use in the operating theater.
The use of mobile phones in healthcare has advantages, for example, the ability to call for other healthcare team members, seek information in medical applications and assisting in learning situations [7,20,28]. What is more, mobile phones are also used for various private purposes during working hours, such as communication, social media, surfing the internet and playing games [17,19,26,28,29]. However, healthcare professionals consider that mobile phones used during work can cause distractions [2,7,18- 20,26,28,29]. All health care categories use their mobile phones at work, but physicians use private mobile phones for professional related tasks more often than nurses do according to research [32]. However, physicians use of mobile phones might be of a professional relation, but it can be questioned how ethical it is to use private cell phones to take pictures of patients for clinical purposes [6,20]. According to Kameda-Smith., et al. (2018) it is common for physicians to store clinical images in private mobile phones and that images are sent via SMS to colleagues. This may jeopardize the patient safety as the identity of the patient might be reveled.
There are also the patient safety issues connected to contamination and the mobility of the Mobil phone. Research shows [4,9,10,11,14-16,21,22,24,30,33,34] that mobile phones are highly contaminated with different types of microorganisms, the most common bacteria being the coagulase-negative staphylococci (KNS). Studies also show the presence of Staphylococcus Aureus (SA) on mobile phones [4,10,11,14,15,24,30,33,34] and methicillin-resistant staphylococci (MRSA) [4,11,15,22-24,33,34]. Cultures from mobile phones also show the presents of other types of bacteria, such as coli bacteria [9,24,33,34], Vancomycin resistant enterococci (VRE) [23], producing extended spectrum beta-lactamase (ESBL) enterobacteria [33], various types of viruses [3,25] and Candida species [13]. The most important patient safety interventions that can be performed to reduce the risk of transmission of microorganisms is to disinfect one’s mobile phone [3,9,25,30]. According to the National Board of Health and Welfare's regulations (Socialstyrelsen) and general advice on basic hygiene in healthcare and social care (2015), healthcare personnel are obliged to apply basic hygiene routines within health- care [31]. Hand disinfection should take place after unclean work, after patient contact and after contact with the patient's immediate environment [8]. One can assume the same relates to disinfection of mobile phones in order to keep a patient safe routine in relation to transmission of bacteria’s in the operating theatre and beyond.
The aim was to describe healthcare professionals use and managing of professional and private mobile phones in the operating theatre.
The design of this study has a descriptive cross-sectional study with structured observations and a questionnaire survey. The study was conducted in three surgical departments at a Swedish children's hospital. The number of observations was pre-determined to 40. Anesthesia nurses, physicians, operating theatre nurses and assistant nurses´ usage of phones in the operating theatre was observed. Included phones were the participants' private mobile phones, operating room fixed telephones and professional mobile phonesused for single or shared use in the operating theatre. Fixed telephones and professional mobile phones are commonly referred to as professional phones in this study. The selection for the observations was carried out in consultation with the department’s operational managers at the observation sessions. The observations were distributed among different operating theatre and operation procedures to include as much diversity as possible. The child´s time in the operating theatre was divided into three stages. 1. Start-up; preparation for the surgery and anesthesia. 2. Surgical intervention; when the surgeon operates on the child. 3. Termination; dressing, control of instruments and materials, anesthesia professionals awakens the child or prepares the intubated child for transportation to the intensive care unit. Each observation lasted one hour and was performed during one or more of these stages. The observer did not know which stage/stages the observations would include until the selection for an observation was performed, which occurred just before the observation sessions. The participants in the questionnaire on private mobile phones in the operating theatre were anesthetic nurses, physicians, operating room nurses and nurses’ assistants. The selection of participants was consecutive. During the survey period, 110 people were on duty at the three departments included.
The contents of the observation protocol and the questionnaire were designed after surveying current studies on the use of professional phones and private mobile phones in the healthcare sector. The observation protocol contained the following variables; number of included healthcare professional in the operating theatre, in what stage of the child's time in the operating theatre as the observations were carried out, time of day - daytime, on-call time, number of uses of professional phones, number of uses of private mobile phones, adherence to basic hand hygiene before use of phones, adherence to basal hand hygiene after use of phones and storage for mobile phones (participants' pockets were excluded). Definitions regarding basic hand hygiene followed the Swedish National Board of Health's (Socialstyrelsen) regulations on basic hygiene in healthcare and social care (2015). The survey began with information on the aim of the study and that consent was given to participate when the questionnaire was answered. The questionnaire consisted of two questions regarding occupation and age, a question regarding desinfecting habits of private mobile phones, and seven questions regarding the use and management of private mobile phones in the operating theatre. The type of questions was closed questions with multiple choice answer options. Prior to the study, three operating theatre nurses piloted the observation protocol. They provided feedback on the contents of the protocol and its function in connection with observations. The questionnaire was piloted by fifteen operating theatre nurses and assistant nurses who provided comments on the content of the questionnaire. The tests led to minor revisions and clarifications in the observation protocol and the questionnaire. The observation protocol and the questionnaire were examined regarding the validity of a specialist nurse holding a PhD degree in nursing.
Prior to the investigation, the head of the clinic and the head of each department's nursing managers were informed about the study. The head of the clinic gave a written consent to conduct the research in the departments. The nursing managers of participating surgical departments informed the staff in writing and verbally about the observations and the questionnaire. Data was collected by conducting structured observations on the use of professional phones and private mobile phones in the operating theatre. The observer had trained to perform the observations according to the observation protocol. During the observations, the observer focused on visible telephones and healthcare professionals who worked in the operating theatre. All observations were made by one person, the first author, and performed in the same manner. The variables were observed for one hour, and every occurrence for a variable was registered in the observation protocol. The questionnaire was available in the departments for 14 days after the observation. The health care workers who had the opportunity to answer the questionnaire were the 110 people who served on the three participating departments during the period in which the study was conducted. After an observation, the number of events was summed up for each variable and the values were recorded in Statistical Package for the Social Science (SPSS) version 24. Data was reviewed to detect unusual values, loss of data or non-existent values. Frequency tables were prepared for each variable and descriptive analysis of data was performed; mean values, medians, standard deviations, minimum and maximum were calculated for data that was ratio scale. Tables were created for some variables.
The present study was a part of a larger study and covered by an approval from the Ethics Review Board in Stockholm (2017/1722- 31/1) regarding research at the participating clinic. Prior to the observations, the participants were informed that it was technical devices that should be observed. The participants were not specifically informed of which technical device the observations concerned. Observing the use and managing of professional phones and private mobile phones meant that the participants' behavior was to some extent investigated, which could lead to participants feeling upset. This risk was discussed in relation to the risk that the participants' use of the phones could change consciously or subconsciously if they knew that technical devices meant professional phones and private mobile phones. Since it was discussed that no studies were carried out in Sweden regarding telephones in the operating theatre and that the present study could provide knowledge that could be of benefit to patients and healthcare professionals. The results in previous studies were discussed as well as the National Board of Health and Welfare's (Socialstyrelsen) regulations and general advice on basic hygiene in health and social care (2015).
The results of the study are based on n=40 observations and n=33 questionnaires.The average number of people in the operating theatre during the observation sessions was 6.8 (median 7). Thirty-five observations were made during the day-time (weekdays 7-16) and 5 observations on on-call time (weekdays after 16, and Saturdays and Sundays). Most observations were made during the stages involving start-up/surgical intervention, 13 observations (32.5%) or during surgical intervention, 10 observations (25%).
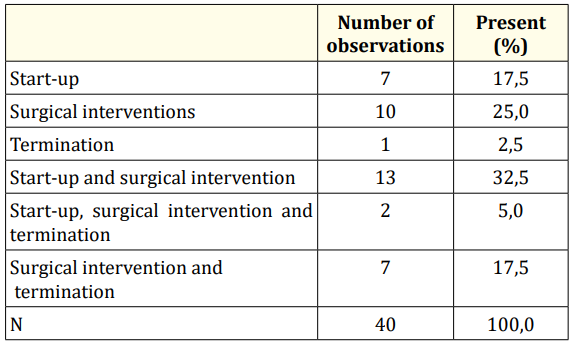
Table 1: Number of observations performed at different stages of the child´s time in the operating theatre.
The number of telephones uses during the observations was 477 - average 11.8, median 12 and standard deviation 5.0. Of the phone usage, 190 (39.8%) was use of professional phones and 287 (60.2%) was use of private phones.
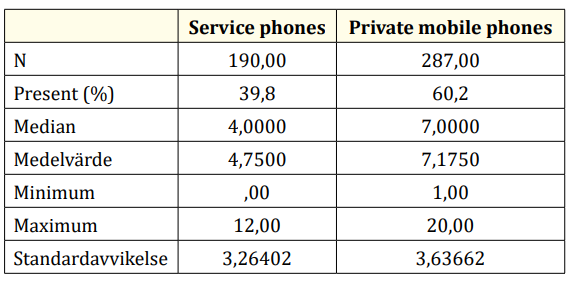
Table 2: Telephone usage, distribution between professional phones and private mobile phones.
The adherence to basal hygiene guidelines before and after telephone use, n = 477, was 93 (19.4%) and 103 (21.5%), respectively. Telephones were used with unclean gloves on 12 occasions, divided into 8 observations.
The most common storage place in the operating theatre for professional phones and private mobile phones (pockets were excluded) were clean tables where 55 phones were stored and computer tables where 48 phones were stored. Forty-three phones were stored in a special place aimed for various types of communication equipment. Thirty-one phones were stored on anesthetic table/anesthetic apparatus and 2 phones on the operating bed. Fifteen phones had other storage places in the operating theatre.
The questionnaire was answered by 33 healthcare professionals. The nonresponse was 77 (70%) of possible participants.
The distribution of occupation in the questionnaire responses was 16 (48.5%) – operating theatre nurses, 8 (24.2%) - assistant nurses, 7 (21.2%) - anesthesia nurses and 2 (6.1%) - physicians. The age distribution was 20 - 34 years - 5 persons (15.2%), 35 - 49 years - 15 persons (45.5%), 50 - 70 years - 13 persons (39.4%).
The result showed that 12 (36.3%) of participants disinfected their private mobile phones every day, 10 (30.3%) weekly and 5 (15.5 %) a few times a month. Two (6%) of the participants disinfected their private mobile phones at fewer occasions than every month and 4 (12.1%) of the participants never disinfected their private mobile phones.
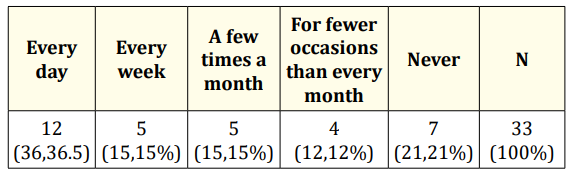
Table 3: Use of private mobile phones for private use in the operating theatre.
Eighteen (54.5%) of respondents replied that they use private cell phones in the operating theatre for contact with their relatives, 9 (27.2%) for pleasure/entertainment and 7 (21.2%) for other private purposes.
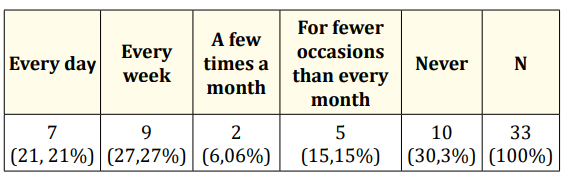
Table 4: Use of private mobile phones for service-related use in the operating theatre
Of the 23 participants who used private mobile phones for service-related use, 20 (86.9%) responded that they searched for information on the internet, 12 (52.1%) used the calculator, 10 (43.4%) medical applications / nursing applications, 8 ( 34.7%) the calendar, 6 (26%) messages, 6 (26.6%), phone calls, 4 (17.3 5) photography and 3 (13 5%) other things.
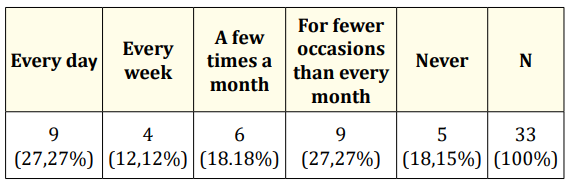
Table 5: Private mobile phones - participants who experienced that the use cause disturbances in the operating theatre.
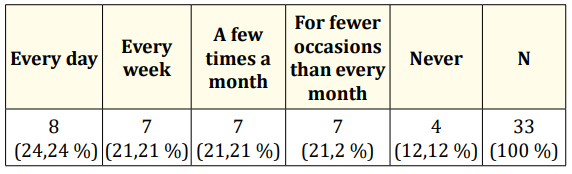
Table 6: Private mobile phones - participants who experienced that the use reduced employee’s concentration.
Eleven (39.3%) of the participants replied that the use of private mobile phones in the operating theatre should be allowed for service-related use, but with restrictions on private use. Ten (33.3%) of participants responded that free use of private mobile phones in the operating theatre should be allowed. Six (18.1%) of participants responded that private mobile phones should not be allowed in the operating theatre.
All studies has limitations and so does our study. The low number of participants from each profession might have contributed to difficulties in diversing between health care workers by profession. Our ambition was to describe healthcare professionals use and managing of professional phones and private mobile phones in the children’s operating theatre. As it is in an everyday situation and not to compare how well different occupation followed guidelines or regulations. Triangulation regarding different data collection methods can increase the validity of an investigation as the different data collection methods can complement each other [27]. Prior to this study, it was considered that observations and a questionnaire could highlight the area from different directions. The observations provided data that might have been difficult to collect with other methods. As the response rate in the questionnaire was low, it was valuable that so much data was obtained during the observations. What is more is the ethical conciderations made prior and during the study that can be criticized. However, according to [27] there is a risk that the participants change their behavior in connection with observations. Participants may want to show a positive image of themselves, which can lead to bias. Because of this, the focus of the observations were not reveled in for hand phones were called technical equipment and during the observations a specific focus were on the mobile phones. From the ethical point of view, the procedure was problematic and ethical discussions were conducted on the issue. There was an awareness that some participants could be upset when the use of private cell phones was investigated. From the result we can show that private mobile phones were used more often in operating theatre than professional phones during the observations. Twelve (36.4%) of the participants replied in the questionnaire that they used mobile phones on a daily basis for private use in the operating theatre and 5 (15.2%) stated that they use the mobile phones for private use in the operating theatre each week. What we do not now from this study is what was considered being of private or professional use. But the results can be compared to studies describing that mobile phones are used for private use at the workplace by more than 75% of healthcare professionals [5,7,17,32]. On the otherhand what is troublesome is that the health-care staff found the use of mobile phones causing desturbances and lack of concentrations, (39.3%) of the participants replied that employees' private mobile phones disturbed every day or every week in the operating theatre. Fifteen (45.5%) of participants had experienced team members to be less concentrated each day or weekly due to the use of private mobile phones. Two of the most reported cauces for patient safety issues. Other researcher has found similar patient safety issues in relation to mobile phones in the operating theatre. [7,29] found that healthcare professionals experience that mobile phones can cause distractions during the health -care work. Surgeons reported disturbances by calls to their own private phones during operations [1,7]. Hygene is also an important patient safety issue that needs concideration in relation to the managing of mobile phones in the operating theatre. Our results questionnaire showed that 4 (12.1%) of participants never disinfected their private mobile phones while 12 (36.3%) responded that they disinfected their private mobile phones every day, which is a higher disinfection rate than in several previous studies. [11] shows that 33.5% of physicians in pediatric care and intensive care never disinfect their mobile phones, but 47% had disinfected their phones in the past week. In a questionnaire survey by [16] regarding the staff's mobile phone habits, it appears that 63% never disinfects their mobile phones, but that 24% disinfects their mobile phones with alcohol daily. One factor that may have contributed to the disinfection frequency being higher in the present study is that 48.5% of the participants in the questionnaire worked as operating theatre nurses. A part of these nurse's area of responsibility includes hygiene. One important factor that was revealed in our study is the compliance to basal hygiene guidelines before and after telephone use, was 19.4% and 21.5%, respectively. [26] shows in a study on mobile phones in operating theatre that 87% of the participants never disinfect their hands after mobile phone use. [25] shows that 28.8% of healthcare professionals in a questionnaire survey never perform hand hygiene before using mobile phones, 37% never perform hand hygiene after using their cell phone and 20.6% do not perform hand hygiene either before or after mobile phone use. The data collection method in this study was observations that were performed during one hour per occasion. In the referenced studies, the participants answered questionnaires regarding hand disinfection habits in connection with telephone use at the workplace. Which implies that our study shows the actual numbers that might correspond to the reality better than the other studies who build their data collection on self reported and estimated information. Could this study in some ways answere the question if mobile phones are d angerous to use or should be prohibited to use in the operating theatre? The result showed that there are diverse opinions among the staff. One reason why the participants had different opinions may be that people are affected in various ways by incidents in the work environment depending on what tasks are performed and what function an individual has in the healthcare team.
Increased adherence to basic hand hygiene guidelines in connection with telephone use can be regarded as important as well as an improved awareness of the advantages and disadvantages of mobile phones usage in operating theatre. Discussing private mobile phone use from an ethical perspective may be important - what is right and wrong with regard to the patients. Another important issue is to analyze why the healthcare professionals use private mobile phones for work related issues instead of using the computers, the mini-calculators and the professional phones that are placed in the operating theatre. There is a need for discussion about whether to bring private mobile phones into the operating theatre, except for those that are necessary for service-related purposes. If private mobile phones are not close at hand, it could possibly be easier to draw the line between mobile phone use for service-related and private use. The private mobile phones that have to be taken into the operating theatre for various reasons can be stored in a special place to reduce use for private purposes and due to hygiene reasons. It can be considered essential to work with guidelines regarding the use of private mobile phones in the operating theatre. Further studies are needed for a continued investigation of the use and managing of mobile phones in the operating theatre.
Copyright: © 2019 Janet Mattsson., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.