Fathi Afshin1, Maskani Reza1* and Hosseini Anbaran Sonia2
1Pediatric Department, Bouali Children’s Hospital, Ardabil University of Medical Sciences (ARUMS), Iran 2Department of Medical, Ardabil Branch, Ardabil University of Medical Sciences (ARUMS), Iran
*Corresponding Author: Maskani Reza, Pediatric Department, Bouali Children’s Hospital, Ardabil University of Medical Sciences
(ARUMS), Iran. Received: October 11, 2019; Published: November 04, 2019
Citation: Maskani Reza. “A Case Report of Giant Cell Rich Osteosarcoma”. Acta Scientific Paediatrics 2.12 (2019):11-13. Giant cell tumor of bone (GCTB) is a benign but locally aggressive bone tumor of young adults. It typically presents as a large lytic
mass at the end of the epiphysis of long bones. Grossly it is comprised of cystic and hemorrhagic areas with little or no periosteal
reaction (1) Giant cell tumor of talus is a rare entity. In contrast to GCT of long bones, most cases occur in a younger age group and
tend to be multicentric (2) we report one case of giant cell rich osteosarcoma of talus bone in a 11 years old Iranian girl in December
2017 that presented with tenderness of the left ankle after a minor trauma with a tumoral lesion in Tc99m-MDP scan. Biopsy of talus
lesion reported a giant cell tumor with focal atypical chondroid and osteoid differentiation highly suggestive of a low grade giant cell
rich osteosarcoma. Neoadjuvant chemotherapy with cisplatin 80mg and Adriamycin 50mg was begin for her Keywords: Giant Cell Tumor; Bone; Osteosarcoma The giant cell tumor of bone (GCTB) is a benign but locally aggressive bone tumor of young adults of 20–40 years of age. It constitutes about 4–5% of all bone tumors and about 18% of all benign
bone tumors. It is slightly more common in females [1] Radiologically, it is usually lytic and expansile without prominent peripheral
sclerosis and periosteal reaction. Some pathologists consider it a
low grade or potentially malignant neoplasm. The tumor is locally
aggressive and destructive, and it tends to recur after simple curetting [1]. GCTB is generally considered a true neoplastic condition with well-defined clinical, radiological and histopathological
features [3,4] Giant cell tumor of talus is a rare entity. In contrast
to GCT of long bones, most cases occur in a younger age group and
tend to be multicentric [2]. A 11-year-old girl presented in December 2016 with one-month
history of left ankle pain after a minor trauma. Radiographs from
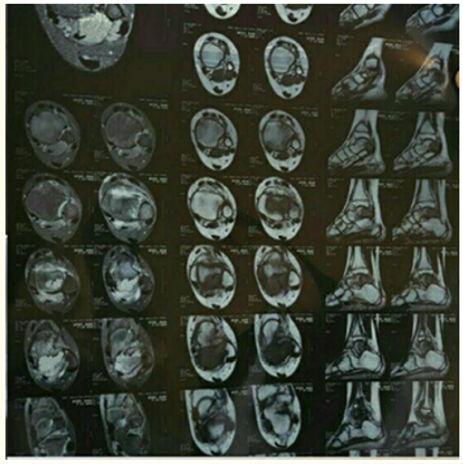
an outside institution showed a cystic lesion in the left ankle (Figure 1). Ankle MRI reported a homogenous well-defined speculated
cystic mass measuring 25*15mm in posterior site of talus with narrow trainsitional zone. Mild joint effusion and soft tissue edema are noted (Figure 2) The patient was undergoing surgery and histopathology report of the lesion was suggestive for solitary bone
cyst with reparative changes following fracture.3 months after surgery the patient's symptoms returned again.in new radiographies
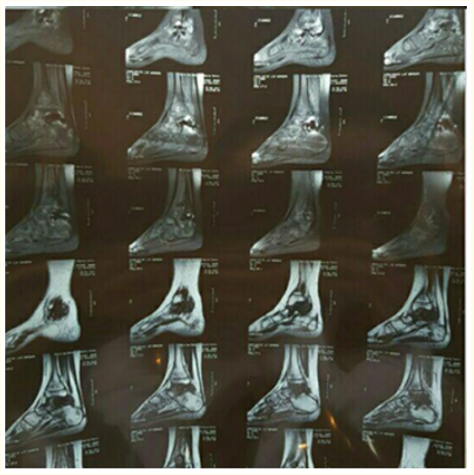
showed a cystic lesion in the left ankle (Figure 1). Figure 1 Figure 2 New MRI reported lateral superior part of talus is dark due
to previous surgery, metallic artifact and sement application. Enhanced distal tibia and talus body and proximal calcaneum are
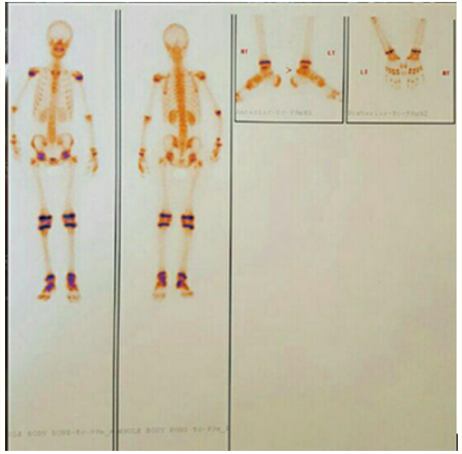
seen as osteitis but no suggestive tumoral tissue is seen (Figure 3). Figure 3 Figure 4 After that whole body scan with injection of the 20mCi Tc99mMDP for patient Was requested and the report was this: the scan finding is suggestive of tumoral lesion in the posterior process of left talus. Increased uptake in the trochlea and neck of left talus can be due to surgical manipulation or extension of tumor. New pathology reported Giant cell tumor with focal atypical chondroid and osteoid differentiation highly suggestive of a low grade giant cell rich osteosarcoma, pending clinico-pathologic and radiologic correlation. Finally giant cell osteosarcoma was diagnosed for patient and neoadjuvant chemotherapy with cisplatin 80mg and Adriamycin 50mg was begin for her last radiography is showed in (Figure 1). Giant cell-rich osteosarcoma is a rarer variant that has very close resemblance to giant cell tumour. Patients usually present nonspecific symptoms of pain and palpable mass. It usually shows an osteolytic lesion with locally spared new bone formation in the metaphysis and/or metaepiphysis on imaging. Histologically, the atypical tumour cells with osteoid formation and multinucleated giant cells are the key factor in the diagnosis and differential diagnosis [5]. Giant cell rich osteosarcomas, histological variant of conventional osteosarcomas account for 3% of all cases of osteosarcomas and most of them are arise from the appendicular skeleton [6]. Giant cell-rich osteosarcomas are sometimes difficult to distinguish from giant cell tumors by age, location, magnetic resonance imaging findings, and pathology. Radiography may be useful in the diagnosis of giant cell-rich osteosarcoma [7]. Malignant giant cell tumor of bone has become a confusing term because of the inclusion of many giant cell-rich sarcomas not related to giant cell tumor of bone (GCT) The term “malignancy in giant cell tumor” may overcome this problem in semantics Malignancy in GCT can be classified as primary when it arises in juxtaposition to a benign giant cell tumor (synchronous malignancy) or secondary when it arises at the site of a previously treated GCT (secondary metachronous malignancy). Most malignancies in GCT are secondary, usually after previous radiation therapy and less commonly after a latent period and previous curettage [8]. In our case, the radiological fining presenting an osteolytic lesion that the scan finding is suggestive of tumoral lesion and highly suggestive of a low grade giant cell rich osteosarcoma. Chest radiography reported no mass lesion and mediastinum, heart shadow size and shape, bone and ribs were normal and patient will be follow after 3 week for second chemotherapy session. Copyright: © 2019 Maskani Reza. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction
Case Presentation
 X
X
 X
X
 X
X
 X
X
Discussion
Bibliography









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.