Vikas Kaushal*
Department of Public Health, Jhpiego, India
*Corresponding Author: Vikas Kaushal, Department of Public Health, Jhpiego, India.
Received: May 29, 2019; Published: July 29, 2019
Citation: Vikas Kaushal. “Pertinent Association between the Immunization and the Nutritional Status in under 5 Children of Urban Slums Area of Karimnagar Town, India”. Acta Scientific Paediatrics 2.8 (2019):61-65.
Background: The prevention of child mortality through immunization is one of the most cost-effective public health interventions in resource deficient settings. Globally, in developing and under developed countries insufficient levels of immunization against childhood diseases remain a major public health problem. The urban average growth rate is 3% while the urban slums growth rate is double at 5-6%. The stark living conditions in slums-characterized by extreme population density, poor sanitation, and a lack of access to basic health services-encourage a host of health challenges.
Objectives: The present study was conducted to determine the status of primary immunization coverage of children ages 1-5 years in urban slums of Karimnagar town, assess the nutritional status of children in that same area and to study morbidity status of children in past one month.
Methods: The Cross-sectional study was conducted in 11 months with children aged 1 to 5 years. The informant was either of the parents or grandparents. WHO Immunization coverage-cluster survey reference manual was used for the calculation of the sample size. Nutritional status was calculated on the basis of BMI, MUAC and IAP classification of malnutrition
Results: According to WHO 30 cluster technique Out of 660, 529 (80.2%) were fully immunized and 131 (19.8%) were partially immunized. This difference of immunization status of children between the religions (χ2=39.384), family types (χ2=42.718), mother’s Knowledge on immunization, distance of immunization center (χ2=310.194) was found to be statistically significant (df=2, p<0.01 and p=0.002, respectively). The relation between low birth weight, malnutrition and sex of child is statistically significant (χ2=24.001, df=4, p<0.001). The relation between immunization status of child and malnutrition and difference of immunization status of children between presences of at least one morbidity condition was also found to be statistically significant (χ2=25.324, df=1, p<0.001).
Conclusion: There is an urgent need to strengthen the existing immunization program among the marginalized communities like those residing in urban slums. Special emphasis should be given to proper and adequate counseling of parents regarding the benefits of immunization.
Keywords: Karimnagar; Immunization; Nutritional Status
The primary objective of immunizing children is to reduce the mortality and morbidity from major illness. It is noteworthy that immunization protects individuals not only from illness per se, but also from the long-term effects of that illness on their physical, emotional and cognitive development [1]. The Expanded Program on Immunization (EPI) was launched with an objective to deliver primary immunization to at least 90% of the infants. Between 1990 and 2015 reduction in child mortality by two-third is the fourth of eight Millennium Development Goals endorsed in 2000. In India Universal Immunization Program was started in 1985 with an aim of achieving at least 85% coverage of primary immunization of infants with 3 doses of DPT & OPV, one dose of BCG & one dose of measles by 1990 [2]. As per National Family Health Survey (NFHS) III data, only 44% of infants in India are fully immunized which is much less than desired goal of 85% and is slightly higher than the coverage as per NFHS II (42%) [3].
Urbanization is a constant growing phenomenon of increasing populations living in cities all over the world but inability to respond to this situation is more in developing countries [4]. The urban average growth rate is 3% while the urban slums growth rate is double at 5-6%. It is projected to inflate to the order of 357 million in 2011 and 432 million by 2021.The stark living conditions in slums-characterized by extreme population density, poor sanitation, and a lack of access to basic health services-encourage a host of health challenges. According to UN-HABITAT (2008/9), “slum dwellers die earlier, experience more hunger, have less education, have fewer chances of employment in the formal sector and suffer more from ill-health than the rest of the inhabitants of cities” [5].
Morbidity in the preschool children residing in the urban slum areas is more as compared to the children in the same age group from higher socioeconomic strata. Unfortunately, malnutrition is rarely perceived as a morbid event by families, communities, and health system [3]. Child malnutrition is the single biggest contributor to under-five mortality due to greater susceptibility to infections and slow recovery from illness. The 3rd National Family Health Survey findings showed that in India 45% of less than3year-old children were malnourished [6]. Therefore, it is necessary to identify specific barriers to scale up immunization coverage in urban slum environments in order to design and improve viable health interventions that will make universal access a realistic possibility. The present study was conducted in the urban slums of Karimnagar town to study the status of immunization coverage and to study the nutritional status of children ages 1 to 5.
Variables regarding the socio demographic details like Parent’s education and occupation have been added. Information about place of delivery and information about routine immunization to parents was made. To evaluate the nutritional status of those children anthropometric measurement was done (weight, height, MUAC), chief complaints, chronic illness, questions regarding their present health status past health status in last one month, disability and deformity were taken.
Ethical clearance was obtained before conducting the study from the Ethical Committee of Prathima Institute of Medical Sciences, Karimnagar. During the survey, verbal consent was taken from the individuals who gave details about their family.
At the end of methodology, continuous variables like age were summarized in terms of descriptive statistics as mean and standard deviation. Categorical variables like socio-demographic details, factors influencing immunization were presented infrequency and percentage. Immunization coverage was computed as percentages. Chi square test of significance was applied to find the association between the factors influencing immunization status and immunization state. A binomial regression analysis was performed to evaluate the various risk factors associated with immunization.
The study was carried out in 30 urban slums of Karimnagar town, taking 22 children from every slum as study sample. The minimum number of families surveyed in each cluster was 12 and maximum was 16 with a mean value of 13.97 ± 1.049 (SD). The age range of children was 14 months to 59 months with mean age of 34.53.
Among the studied population 660 (100%) had received BCG 616 (93.3%), receivedOPV0 660 (100%), received OPV1 648 (98.2%), received OPV2 581 (88%), received OPV 3 660 (100%), received DPT 1 648 (98.2%), received DPT2648 (98.2%), received DPT3 581 (88%), received Measles 583 (88.3%) (Figure1). Among the surveyed children 529 (80.2%) were fully immunized and 131 (19.8%) were partially immunized. Our finding is incoherent with NFHS result [6-11] because of selection of heterogeneous clusters and improved immunization facility in last 10 years.
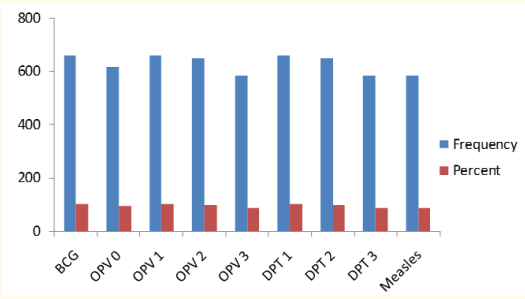
Figure 1: Distribution of vaccination status in the context of primary vaccines.
The children in the study were distributed religion wise on the basis of their immunization status and it was found that the immunization status of children between the religions was statistically significant (χ=39.384, df=2, p< 0.01) (Table 1). The religion and family type distribution of children in relation to their immunization status was also studied. This difference of immunization status of children between the religions (χ=39.384, df=2, p < 0.01, Figure 2) and family type (χ=42.718, df=2, p < 0.001, Figure 3) was found to be statistically significant. The results of our study were comparable to study done by Chaudhary., et al. (2010), where 67.5% Hindus were fully immunized and among Muslims, 44% were fully immunized and by Vilas R., et al. (2013) 81.44% Hindu children were fully immunized and 74.19% Muslim children were fully immunized.
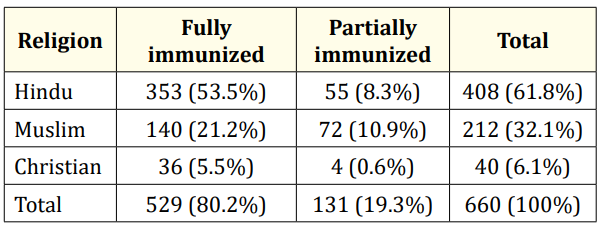
Table 1: Religion wise distribution of children by immunization status.
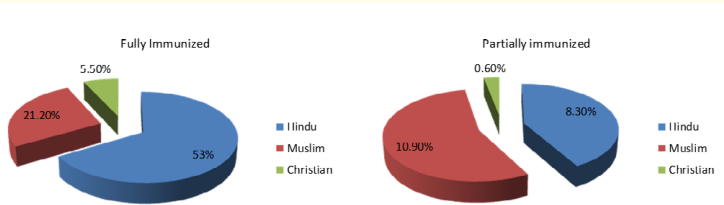
Figure 2: Religion wise distribution of children by their immunization status.
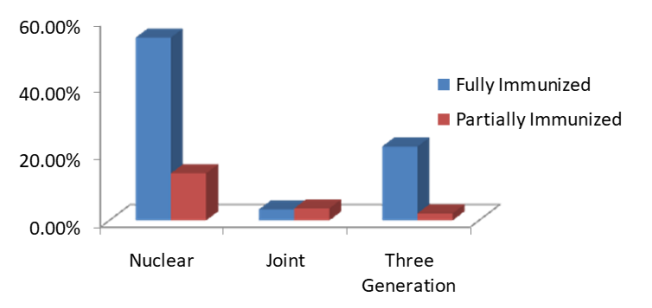
Figure 3: Distribution of family type of children in relation to Immunization status.
In the present study we also evaluated the malnutrition status in children aged more than 24 month on the basis of BMI and it was found that 275 (60.7%) were underweight while 178 (39.3) were healthy weight (Table 4). On the basis of MUAC 204 (30.9%) found to be well nourished, 200 (30.3%) were at risk for malnutrition, 245 (37.1%) were moderately acute malnourished while 11 (1.7%) were severely acute malnourished according to findings of mid upper arm circumference measurement (Figure 4a). The results of our study was in line with the study conducted by Das., et al. (2014), where the prevalence rate of mild malnutrition was 30.20% and severe malnutrition was 2.20%.
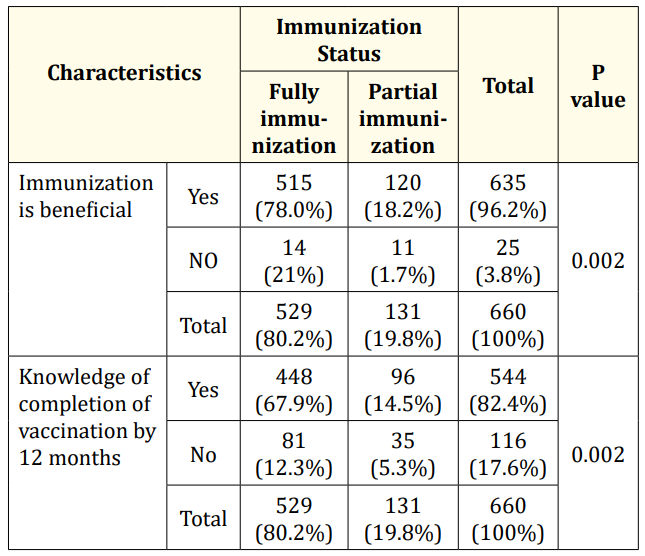
Table 2: Knowledge of immunization among mothers in relation to immunization status.
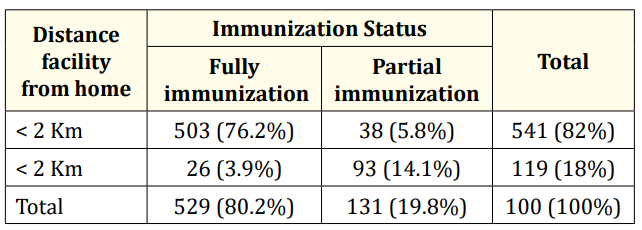
Table 3: Relationship of immunization status in relation with distance of health facility.
In the present study we also evaluated the malnutrition status in children aged more than 24 month on the basis of BMI and it was found that 275 (60.7%) were underweight while 178 (39.3) were healthy weight (Table 4). On the basis of MUAC 204 (30.9%) found to be well nourished, 200 (30.3%) were at risk for malnutrition, 245 (37.1%) were moderately acute malnourished while 11 (1.7%) were severely acute malnourished according to findings of mid upper arm circumference measurement (Figure 4a). The results of our study was in line with the study conducted by Das.,et al. (2014), where the prevalence rate of mild malnutrition was 30.20% and severe malnutrition was 2.20%.
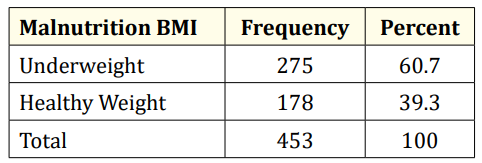
Table 4: Malnutrition based on BMI.
According to Indian Academy of Pediatrics weight for age it was found 164 (24.85%) children were normal. Under grades of mild, moderate, severe and very severe malnourished the number of children were 227 (34.39%), 177(26.82%), 57 (8.64%) and 35 (5.3%) respectively (Figure 4b). It was further evaluated that relationship of malnutrition was statistically significant (p < 0.001) to low birth weight, sex of child and immunization status (Table 5a, b and c) which indicated that vaccination provides protection against morbidity and this in long run improves nutrition status as repeated illness leads to deterioration of health.

Table 5a: Relationship of malnutrition with LBW.

Table 5b: Relationship of malnutrition with sex of child.

Table 5c: Relationship of malnutrition with immunization status.
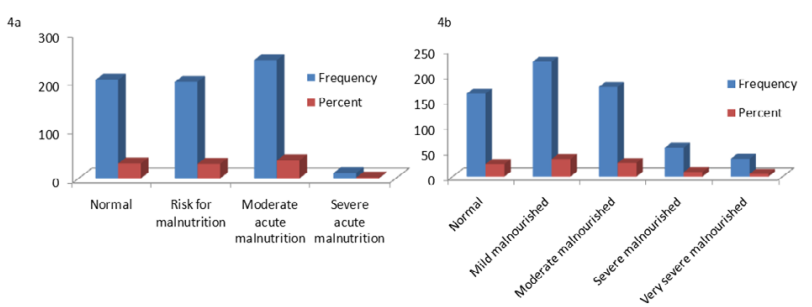
Figure 4: Malnutrition grading according to (4a) MUAC and (4b) IAP.
In the present study it was observed that, 50.9% were male and 49.1% were female children with a mean age of 13.97 month. The information was acquired from father (19.8%), mother (75.9%) and grandparents (4.3%). Maximum were of 1st and 2nd birth order i.e. 43.2% and 44.4% respectively, rest 12.4% were of 3rd birth order. Among subjects 61.8% were Hindus, 32.1% of Muslims and 6.1% were Christian. Maximum belonged to upper lower class 64.7% and only 1.7% belonged to upper class and 2% belonged to lower class, generally from nuclear family (68.8%). The maximum educational qualification of mother with a mean age of 23.79 years was high school 39.7% and minimum honors were 1.7%. Most of the mothers were home maker (81.8%), only 4.1% were semiskilled and 2% were skilled workers. Related to the literacy status of fathers 35.9% were illiterate and 1.8% honors. Immunization card was available of 92.9% children. The overall immunization status of the children found in the study was 80.2% fully immunized and 19.8% partially immunized with 100% BCG, OPV1 and 77 DPT1 coverage. Reasons for partial and non-immunization were categorized as – child illness (58.77%), Unawareness of need of immunization (9.92%), Lack of time or busy in other work (9.16%) , Away from home at the time of immunization (22.13%) .The association between socio demographic variables like sex, birth order, religion, family type, education of father, knowledge and attitude of mother and distance of immunization facility from home and the immunization status were not found to be statistically significant among these children. According to MUAC classification of malnutrition 40.9% children were malnourished and 59.1% not malnourished. In accordance to IAP classification of malnutrition, 24.85% children were normal, 34.39% were grade 1, 26.82% were grade 2, 8.64 grade 3, 5.30% grade 4 malnourished respectively. The association between LBW, sex of child and immunization status were found to be significant among children. Amongst children 63.9% were presented with at least one morbidity condition and its relation with immunization status was also found to be significant.
Copyright: © 2019 Vikas Kaushal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.