Swapan Kumar Chowdhury1*, Shafi Ahmed2, Israt Ara Hossain3, Rabeya Yasmin4, MH Faruquee5 and AFM Salim6
1PhD Fellow, Bangladesh University of Professionals, Dhaka, Bangladesh
2Associate Professor, Department of Pediatrics, Khwaja Yunus Ali Medical College and Hospital Enayetpur, Sirajgonj, Bangladesh
3Senior Lecturer, Department of Biochemistry and Cell Biology, Bangladesh University of Health Sciences, Dhaka, Bangladesh
4Assistant Professor, Department of Occupational and Environmental Health, Bangladesh University of Health Sciences, Dhaka, Bangladesh
5Associate Professor, Department of Occupational and Environmental Health, Bangladesh University of Health Sciences, Dhaka, Bangladesh
6Ex-Professor, Institute of Child Health and Shishu Swasthya Foundation Hospital, Mirpur, Dhaka, Bangladesh
*Corresponding Author: Swapan Kumar Chowdhury, PhD Fellow, Bangladesh University of Professionals, Dhaka, Bangladesh.
Received: May 20, 2019; Published: July 02, 2019
Citation: Swapan Kumar Chowdhury., et al. “Status of Iron Deficiency Anemia among Bangladeshi Children: Urban and Rural Settings”. Acta Scientific Paediatrics 2.8 (2019):08-12.
Iron deficiency (ID) is the most common nutritional deficiency in the world and infants and young children are at the highest risk. Poor school performance, lessen work capacity, increase susceptibility to infections, impaired growth, and mental retardation are the long term consequences of anemia. This study was a part of a community based cross sectional study which was conducted among 274 children from two primary schools (one from Dhaka city and one from Gazipur district). The male and female ratio was equal. The mean age of the students was 8.86 ± 2.035 years. Majority of the children were within 5 - 10 years (73.7%) and rest were within 10 - 14 years. Among the study participants 48.2% were of rural areas and 51.8% were from urban area. Venous blood was collected by trained phlebotomist. Estimation of serum Hemoglobin was measured in a spectrophotometer at a wavelength of 540 nm. Serum Iron analysis was done singly as part of Multi-analytic Biochemistry Panel using Beckman Synchron LX20 in a reference laboratory. The mean hemoglobin was 11.89 ± 1.55 among the rural subjects and 11.55 ± 0.96 among the urban subjects. While mean hemoglobin was 11.87 ± 1.29 among the male subjects and 11.56 ± 1.29 among the female subjects. Statistically significant differences were found between rural and urban and male and female subjects (p<0.05). Serum iron level was estimated which shows that all the subjects had below 50 µg/dl. Overall prevalence of anemia and insufficiency serum iron among the school going children is marked and needs to explore the root cause.
Keywords: Serum Iron; Children; Urban and Rural Settings; Bangladesh
Around 1.62 billion people corresponds to one-fourth of the population in the world are suffering from anemia [1]. World Health Organization (WHO) reported that about 246.4 million under five and 46% of 5- 14 years old children are anemic. Prevalence was reported higher among female than male adolescent [2-4]. Anemia prevalence is ranking more than forty percent as high; fifteen to forty percent as medium; and less than fifteen percent as low [5]. The proportion of anemia associated with iron deficiency was lower in countries where anemia prevalence was >40%, especially in rural populations (14% for pre-school children), and in countries with very high inflammation exposure (20% for pre-school children) [6]. In Bangladesh prevalence of anemia among schoolage children is 30-40% [7]. Poor school performance, lessen work capacity, increase susceptibility to infections, impaired growth, and mental retardation are the long term consequences of anemia [8]. Anemia is still now being one serious public-health problem in Bangladesh. Around 46% of under-five children are suffering from anemia [9,10]. Therefore, this cross-sectional study was an attempt to explore the status of hemoglobin and iron deficiency among school going children in Bangladesh.
This study was a part of a community based cross sectional study which was conducted among 274 primary school children during March 2018 to February 2019. Two primary schools were selected purposively (one from Dhaka city and one from Gazipur district). After taking written informed consent from guardians all required data were collected. Data components were about socio-demographic information, anthropometric measurement and biological sample collection and serum iron measurement. At the time of enrollment, trained research assistants administered a pretested socio-demographic questionnaire of each participating subject. Socio-demographic information including age, household size, education of parents or caregiver, income, employment of the head of the households and housing condition were recorded. Venous blood was collected in the morning taking after a 4 -6 hour overnight fast by trained phlebotomist. Samples were taken in the red-top tube for serum separator. Then the tubes were kept in cold box and sent to the reference laboratory within 4 h. For Hemoglobin estimation, blood was diluted in a solution containing potassium cyanide and potassium ferricyanide. The absorbance of the solution was then measured in a spectrophotometer at a wavelength of 540nm or in a colorimeter using a yellow green filter. For serum Iron analysis, the sample volume for individual test, 25 µl was added to 210 µl of reagent. Sample was run singly as part of Multi-analytic Biochemistry Panel.
Only borosilicate glass containers were used to store samples. The Serum Iron was tested through using Beckman Synchron LX20 in a reference laboratory. ID was defined as TBI < 0 mg/kg. Anemia was defined as hemoglobin concentration <11.0 g/dL. IDA was defined as having both anemia and ID. Estimates were weighted and take into account NHANES complex survey design. We used chi square tests to assess whether prevalence estimates varied by age.
Among the study participants, male female ratio was equal. The mean age of the study subjects were 8.86 ± 2.035 years. Majority of the children were within 5 - 10 years (73.7%) and rest were within 10 - 14 years. The male and female ratio was equal. Among the participants 28.8% were in class I, 20.1% were in class II, and 16.4% were in class III, 17.9% in class IV and rest 16.8% were in class V. Around 48% study participants were of rural areas (Table 1,2).
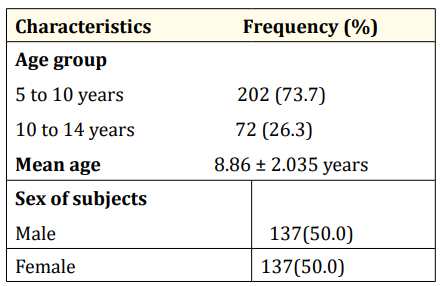
Table 1: Socio-demographic distribution of subjects (n=274).
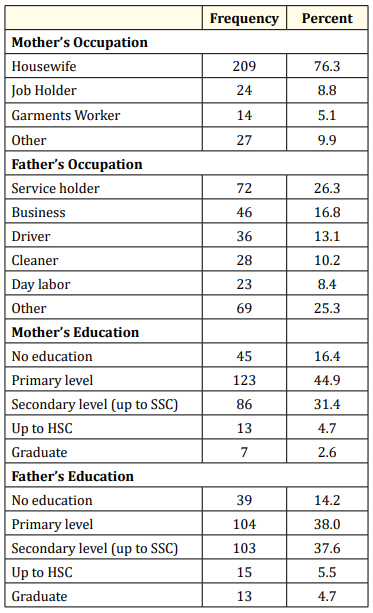
Table 2: Distribution of respondents by socio-demographic characteristics.
Among the mothers of the subjects, 76.3% were housewife while rest were found engaged with individual profession. Among the fathers 26.3% were service holder, 16.8% were engaged with business and rest were found engaged in different profession. The education level of the mothers were found as 16.4% had no institutional education, 44.9% had primary level, 31.4% had secondary level (up to SSC), 4.7% had up to HSC level and 2.6% were graduate. That of father was found as 14.2% had no institutional education, 38.0% had primary level, 37.6% had secondary level (up to SSC),
5.5% had up to HSC level and 4.7% were graduate.
The table 3 shows that among the rural subjects, 6.8% had Hemoglobin level within 7-9.9, 23.5% had within 10- 10.9, and 69.7% had 11 and above level. Among the urban subjects. 2.8% had Hemoglobin level within 7-9.9, 25.4% had within 10- 10.9, and 71.8% had 11 and above level. On the other hand among the male subjects 3.6% had Hemoglobin level within 7-9.9, 20.4% had within 10- 10.9, and 75.9% had 11 and above level. Among the female subjects. 5.8% had Hemoglobin level within 7-9.9, 28.5% had within 10- 10.9, and 65.7% had 11 and above level. No statistically significant difference were found between urban and rural subjects and male and female subjects as well (p>0.05).
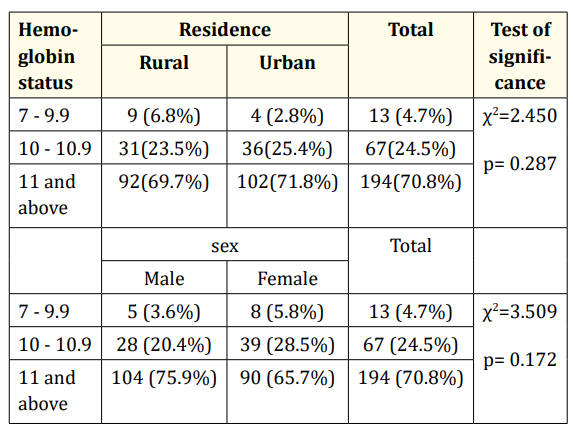
Table 3: Distribution of subjects by serum Hemoglobin status by area of residence and sex.
Serum iron level was estimated which shows that all the subjects had below 50 µg/dl (Table 4).
The mean hemoglobin was 11.89 ± 1.55 µg/dl among the rural subjects and 11.55 ± 0.96 µg/dl among the urban subjects. While mean hemoglobin was 11.87 ± 1.29 µg/dl among the male subjects and 11.56 ± 1.29 µg/dl among the female subjects. Statistically significant differences were found between rural and urban and male and female subjects (p<0.05) (Table 5).
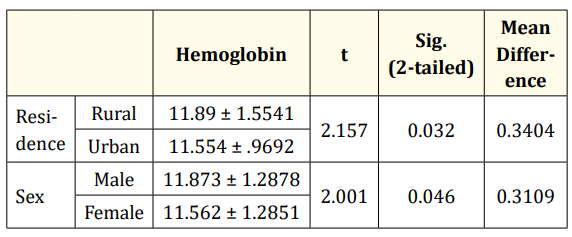
Table 4: Serum Hemoglobin status by area of residence and sex.
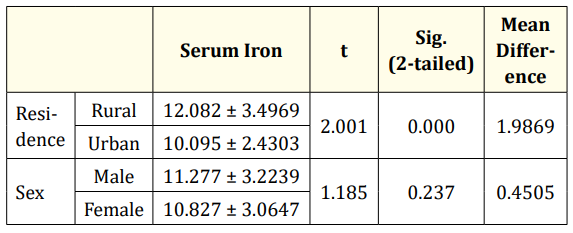
Table 5: Serum Iron status by area of residence and sex.
The mean serum iron was 12.08 ± 3.50 µg/dl among the rural subjects and 10.09 ± 2.43 µg/dl among the urban subjects, while the mean serum iron was 12.05 ± 3.49 µg/dl among the male subjects and 10.09 ± 2.43 µg/dl among the female subjects. Statistically significant differences were found between rural and urban subjects (p<0.05) but not between male and female (p>0.05).
The study was conducted among the primary school students of rural and urban settings. This current study included a total 274 children of whom 132 were from rural area and 142 were from urban area with equal male female ratio. Among the subjects, seventy four percent were in the age group of 5 to 10 years age followed by twenty six percent were in the age group of 10 to 14 years of age with mean 8.86 ± 2.035 years. Among the mothers of the subjects, seventy six percent were housewife while rest were found engaged with individual profession. Among the fathers more than one-fourth were service holder, seventeen percent were engaged with business and rest were found engaged in different profession. The education level of the mothers, around sixteen percent had no institutional education, forty five percent had primary level, and thirty one percent had secondary level (up to SSC) of education. And that among the father, fourteen percent had no institutional education, thirty eight percent had primary level, around same percent had secondary level (up to SSC) education.
This current study suggests that urban students were significantly heavier than rural students as judged by their weight, BMI, HAZ and WHZ (p < 0.05). While no such difference were found among the male and female students.
Among the study subjects Serum iron level was estimated which shows that all the subjects had below 50 µg/dl. The mean hemoglobin was 11.89 ± 1.55 among the rural subjects and 11.55 ± 0.96 among the urban subjects. While mean hemoglobin was 11.87 ± 1.29 among the male subjects and 11.56 ± 1.29 among the female subjects. Statistically significant differences were found between rural and urban and male and female subjects (p<0.05). The mean serum iron was 12.08 ± 3.50 among the rural subjects and 10.09 ± 2.43 among the urban subjects, while the mean serum iron was 12.05 ± 3.49 among the male subjects and 10.09 ± 2.43 among the female subjects. Statistically significant differences were found between rural and urban subjects (p<0.05) but not between male and female (p>0.05). Study in Kerala India [11] the mean serum iron was 64.60 ± 20.30 μg/dl., in Punjab [12] found 97% of the study school-children (11-17 years) anemic, in Odisha [13] 8%, in Pune [14] among the adolescent schools girls 56% of urban and 63% of rural were suffering from anemia, are anemic. The mean haemoglobin level among rural and urban adolescent were 10.53 gm% and 10.44% respectively. In Equatorial Guinea, over 85% were anemic especially in rural area. While in Ethiopia [15] the prevalence of anemia was 11.1% among school going adolescent girls in rural area and in Pakistan [16] 12.7% male and 30.4% female were anemic (mean Hb level 11.1 ± 4.94). In Bangladesh [17], one study among university students found that 55.3% were anaemic (Male- 36.7% and Female 63.3%).
Iron deficiency itself seemed to be more prominent problem. It most often occurs as result of inadequate iron intake. Among young child, low iron content of milk and other preferred food, and also rapid growth rate can cause iron deficiency. Another cause of iron deficiency may be over cooking of food among the study population as observed by the researcher. The other possible mechanism of decrease in serum iron level is due to elevated needs and chronic loss from parasitic infections. Diarrhea and other infections can cause malnutrition through decreased nutrient absorption, decreased intake of food, increased metabolic requirements, and direct nutrient loss [18]. Another mechanism for decreased iron is majority of dietary non-haem iron enters the gastrointestinal tract in the ferric form. However, Fe3+ is thought to be essentially non-bioavailable and therefore, it must first be converted to ferrous iron prior to absorption. There are numerous dietary components capable of reducing Fe3+ to Fe2+, including ascorbic acid, and amino acids such as cysteine and histidine [19].
Overall prevalence of anemia and insufficiency of serum iron among the school going children is marked and needs to explore the root cause.
The authors greatly acknowledge Department of Biochemistry, Bangladesh University of Health Sciences for providing laboratory facilities. The teachers and guardians of the participants are also highly acknowledged.
Authors declare that they have no conflict of interest.
Copyright: © 2019 Swapan Kumar Chowdhury., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.