Shafi Ahmed1*, Swapan Kumar Chowdhury2, Israt Ara Hossain3, Rabeya Yasmin4, Muhammad Mozammel Haque5, MH Faruquee6 and AFM Salim7
1Associate Professor, Department of Pediatrics, Khwaja Yunus Ali Medical College and Hospital Enayetpur, Sirajgonj, Bangladesh
2PhD Fellow, Bangladesh University of Professionals, Dhaka, Bangladesh
3Senior Lecturer, Department of Biochemistry and Cell Biology, Bangladesh University of Health Sciences, Dhaka, Bangladesh
4Assistant Professor, Department of Occupational and Environmental Health, Bangladesh University of Health Sciences, Dhaka, Bangladesh
5Consultant Pediatrics, Mahbubur Rahman Memorial Hospital and Nursing Institute, Rupashdi, Banchharampur, Brahmanbaria, Bangladesh
6Associate Professor, Department of Occupational and Environmental Health, Bangladesh University of Health Sciences, Dhaka, Bangladesh
7Ex-Professor, Institute of Child Health and Shishu Swasthya Foundation Hospital, Mirpur, Dhaka, Bangladesh
*Corresponding Author: Shafi Ahmed, Associate Professor, Department of Pediatrics, Khwaja Yunus Ali Medical College and Hospital, Enayetpur, Sirajgong, Bangladesh.
Received: May 20, 2019; Published: July 02, 2019
Citation: Shafi Ahmed., et al. “Status of Serum Vitamin D among Bangladeshi Children: Urban and Rural Settings”. Acta Scientific Paediatrics 2.8 (2019):03-07.
Vitamin D plays role in regulating cell growth, maintenance of body immunity, healthy musculoskeletal structure and functioning other various biological activities in keeping people healthy. This study was a part of a community based cross sectional study which was conducted among 274 primary school children. Two primary schools were selected purposively (one from Dhaka city and one from Gazipur district). The male and female ratio was equal. The mean age of the students was 8.86 ± 2.035 years. Majority of the children were within 5 – 10 years (73.7%) and rest were within 10 – 14 years. The male and female ratio was equal. Among the participants 28.8% were in class I, 20.1% were in class II, and 16.4% were in class III, 17.9% in class IV and rest 16.8% were in class V. Among the study participants 48.2% were of rural areas and 51.8% were from urban area. Standardized anthropometric measurements of body weight and height were made by trained nurses. Venous blood was collected by trained phlebotomist. Estimation of serum vitamin D was done in one reference laboratory. It was found that 60.6%rural respondents had below 20 ng/ml of serum Vitamin D, while none of urban children had below 50ng/ml of Serum Vitamin D. Mean value is significantly different between rural and urban children (p < 0.05). On the other hand 26.3% of male and 32.1% female children had Serum Vitamin D below 20 ng/ml. No such statistical difference was observed between male and female. The prevalence of vitamin D deficiency and insufficiency especially among rural school going children in Bangladesh is very high and alarming which needs to explore the root cause.
Keywords: Serum Vitamin D; Children; Urban and Rural Settings; Bangladesh
Vitamin D plays role in regulating cell growth, maintenance of body immunity, healthy musculoskeletal structure and functioning other various biological activities in keeping people healthy [1- 4]. Deficiency of Vitamin D has commonly been reported among people suffering from chronic pain which raise the question of its relationship [5-9]. American endocrinologist Holick mentioned that deficiency of Vitamin D might be the causes of muscular weakness and muscle pain among children and adults as well [10,11]. Persistent and nonspecific musculoskeletal pain has been observed at high risk by scientists due to unrecognized and untreated severe deficiency of Vitamin D [12].
Nutrition plays a vital role in the proper growth and development for children. Unfortunately, one child cannot receive enough vitamin D from dietary sources alone. Instead, like adults, children must rely on sunshine and supplements to maintain healthy vitamin D levels [13]. Deficiency of Vitamin D is now a day’s been identified as the evidence of lifestyle disorder in the urban population even after abundant sunlight. They fail to expose themselves to sunlight due to long school time, lack of physical activities and exercises [14]. The study is an attempt to find out the blood vitamin D statuses among Bangladeshi children: Urban and Rural setting.
This study was a part of a community based cross sectional study which was conducted among 274primary school children during March 2018 to February 2019. Two primary schools were selected purposively (one from Dhaka city and one from Gazipur district). After taking written informed consent from guardians all required data were collected. Data components were about sociodemographic information, anthropometric measurement and biological sample collection and serum vitamin D measurement. At the time of enrollment, trained research assistants administered a pretested socio-demographic questionnaire of each participating subject. Socio-demographic information including age, household size, education of parents or caregiver, income, employment of the head of the households and housing condition were recorded. Standardized anthropometric measurements of body weight (W) and height (H) were made by trained nurses. The measurements were expressed as Z scores for H/A and W/H (height/age and weight/height), which are the differences between the child's weight and height. All the estimates of wasting, underweight, and stunting amongst children have been done using standard computer software, severe acute malnutrition is defined as <-3z scores weight-for-height and/or oedema. Anthropometric data were analyzed by NCHS standard for the classification of malnutrition. For reporting of height for age, weight for age and weight for height relative to the NCHS reference percentile and Z-score was used [15]. Venous blood was collected in the morning taking after a 4 -6 hour overnight fast by trained phlebotomist. Samples were taken in the red-top tube for serum separator. Then the tubes were kept in cold box and sent to the reference laboratory within 4 h. Serum Vitamin D was measured using an electro-chemiluminescence enzyme immunoassay method (ADVIA Centaur; USADPC Co., USA, according to manufacture instructions.
Among the study participants, male female ratio was equal. The mean age of the study subjects were 8.86 ± 2.035 years. Majority of the children were within 5 – 10 years (73.7%) and rest were within 10 – 14 years. The male and female ratio was equal. Among the participants 28.8% were in class I, 20.1% were in class II, and 16.4% were in class III, 17.9% in class IV and rest 16.8% were in class V. Around 48% study participants were of rural areas.
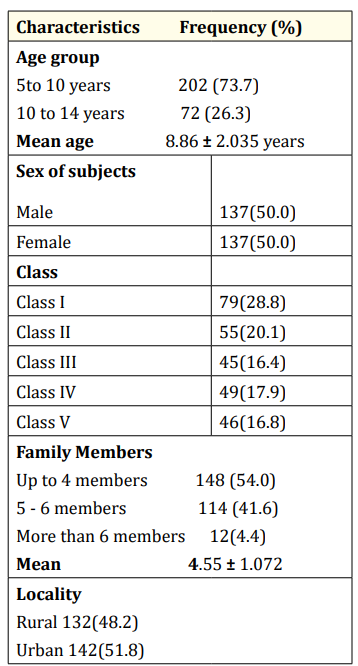
Table 1: Socio-demographic distribution of subjects (n=274).
Among the mothers of the subjects, 76.3% were housewife while rest were found engaged with individual profession. Among the fathers 26.3% were service holder, 16.8% were engaged with business and rest were found engaged in different profession. The education level of the mothers were found as 16.4% had no institutional education, 44.9% had primary level, 31.4% had secondary level (up to SSC), 4.7% had up to HSC level and 2.6% were graduate.

Table 2: Distribution of respondents by socio-demographic characteristics.
That of father was found as 14.2% had no institutional education, 38.0% had primary level, 37.6% had secondary level (up to SSC), 5.5% had up to HSC level and 4.7% were graduate.
The table 3 shows that among the study population, urban students were significantly heavier than rural students as judged by their weight, BMI, HAZ and WHZ (p < 0.05). While no such difference were found among the male and female students.

Table 3: Anthropometric characteristics of school going children: Rural-Urban and Male-Female Settings. HAZ, Height for age Z score; WAZ, Weight for age Z score; WHZ, Weight for Height Z score, BMI, Basal Metabolic Index, All values are mean ± SD
The table 4 shows that the Serum Vitamin D was 18.899 ± 10.15 ng/ml (60.6% below 20 ng/ml) among the rural school children and 171.088 ± 94.74 ng/ml among the urban children (none is below 50ng/ml). Mean value is significantly different between rural and urban children (p < 0.05). While same was 93.757 ± 102.70ng/ ml (26.3% below 20 ng/ml) among the male children and 101.784 ± 102.35 ng/ml (32.1% below 20 ng/ml) among the female children. No such statistical difference was observed between male and female.

Table 4: Serum Vitamin D status by area of residence and sex.
The study was conducted among the primary school students of rural and urban settings. This current study included a total 274 children of whom 132 were from rural area and 142 were from urban area with equal male female ratio. Among the subjects, seventy four percent were in the age group of 5 to 10 years age followed by twenty six percent were in the age group of 10 to 14 years of age with mean 8.86 ± 2.035 years. Among the mothers of the subjects, seventy six percent were housewife while rest were found engaged with individual profession. Among the fathers more than one-fourth were service holder, seventeen percent were engaged with business and rest were found engaged in different profession. The education level of the mothers, around sixteen percent had no institutional education, forty five percent had primary level, and thirty one percent had secondary level (up to SSC) of education. And that among the father, fourteen percent had no institutional education, thirty eight percent had primary level, around same percent had secondary level (up to SSC) education.
This current study suggests that urban students were significantly heavier than rural students as judged by their weight, BMI, HAZ and WHZ (p < 0.05). While no such difference were found among the male and female students.
Vitamin D deficiency is a global public-health concern, even in tropical regions where the risk of deficiency was previously assumed to be low due to cutaneous vitamin D synthesis stimulated by exposure to sun. The current study observed that the mean value of Serum Vitamin D is significantly more among urban children than that of rural children (p < 0.05), while no such statistical difference was observed between male and female. Among the rural school children 60.6% had serum Vitamin D below 20 ng/ml and among the urban children none had below 50ng/ml. While among the male children 26.3% had serum Vitamin D below 20 ng/ml and 32.1% female children had below 20 ng/ml. Severe vitamin D deficiency as observed in our study population has also been reported in Bangladesh and India [16]. Though Vitamin A deficiency was reported prevalent among 8% of school-age children in Bangladesh and 26% of male children in Sri Lanka by Akhtar and associates [17]. Another study conducted in Bangladesh very nearer to this study area showed that among the 6 - 11 years children, 41.02% were deficient and 52.56% were insufficient of vitamin D-deficient [18]. As conservative clothing practices (i.e. veiling) and low frequency of intake of foods from animal source (other than fish) were common among the rural people in Bangladesh may be one of the predisposing factor of vitamin D deficiency. This statement is supported by Holick and Chen [19].
The prevalence of vitamin D deficiency and insufficiency especially among rural school going children in Bangladesh is very high and alarming which needs to explore the root cause.
The authors greatly acknowledge Department of Biochemistry, Bangladesh University of Health Sciences for providing laboratory facilities. The teachers and guardians of the participants are also highly acknowledged.
Authors declare that they have no conflict of interest.
Copyright: © 2019 Shafi Ahmed., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.