Sagar A Jawale*
Jawale Institute of Pediatric Surgery, Jalgaon- Maharashtra, India
*Corresponding Author: Sagar A Jawale, Jawale Institute of Pediatric Surgery, Jalgaon- Maharashtra, India.
Received: April 29, 2019; Published: June 26, 2019
Citation: Sagar A Jawale. “Tongue Tie Release Operation (Frenotomy) By Methylene Blue Dye Induced Infrared Laser Cutting”. Acta Scientific Paediatrics 2.7 (2019):26-29.
Introduction: Tongue-tie (ankyloglossia) is a common congenital anomaly in children with incidence of 4.8% of live births. With tongue-tie, an unusually short, thick or tight band of tissue (lingual frenulum) tethers the bottom of the tongue's tip to the floor of the mouth, so it may interfere with breast-feeding, speech, eating, swallowing. The standard surgical treatment offered to this congenital anomaly is Frenotomy operation. I describe a new and unique surgical treatment option for this anomaly which is described for the first time in medical literature.
Materials and Methods: In last 3 years in Jawale Institute of pediatric surgery, I did 21 cases of Tongue Tie release operation (Frenotomy) with methylene blue dye induced infrared laser cutting technique (Group A). 26 patients during same period were put as control (Group B) where the Frenotomy operation was done with conventional technique with electrocautery.
Conventionally, frenotomy is performed under general anesthesia with cutting type of electrocautery to lengthen the tongue till it comfortably comes out of mouth. In my technique of Tongue tie release operation (Frenotomy) is done by injecting methylene blue dye into frenulum and cutting it by infrared laser of 950 nm and 20 Watt in power. Methylene blue has the opposite color of infrared, hence maximum absorption and cutting occurs.
Results: In group A, 1(4.76%) patient complained difficulty in eating and swallowing, 2 patients (9.52%) had pain postoperatively for more than 48 hours. No patient had edema of tongue. There was no postoperative bleeding. In Group B, 6(23.07%) patients complained difficulty in eating and swallowing, 12(46.15%) patients had pain postoperatively for more than 48 hours. 6 (23.07%) patients had edema of tongue and 2(7.69%) patients had mild oozing of blood after 48 hours.
Discussion: In The advantages of this technique over the conventional are as follows. The operation is blood less as the infrared laser of 950 nm has a much better coagulation power compared to the electrocautery. As the laser is quite precise, the collateral damage produced by laser is much lower compared to electrocautery. Because of the Methylene blue dye a cheap infrared laser (USD 500) can be used for this purpose. Otherwise, a high frequency 2000 nm and high wattage (40 Watt) laser has to be used which is extremely costly (USD 50,000) and is not affordable to most surgeons. Methylene blue as a dye that is already FDA approved to be used topically as well as intravenously in human body. Hence there are no ethical issues for using it on human body. This new and unique surgical treatment option for this anomaly which is described for the first time in medical literature.
Conclusions: The Tongue tie release operation (Frenotomy) by methylene blue dye induced infrared laser is a safe, effective and affordable technique. The technique can be used on plenty of other operations in surgery.
Keywords: Tongue; Frenotomy; Laser
Tongue-tie (ankyloglossia) is a common congenital anomaly in children with incidence of 4.8% of live births [1]. With tongue-tie, an unusually short, thick or tight band of tissue (lingual frenulum) tethers the bottom of the tongue's tip to the floor of the mouth, so it may interfere with breast-feeding. Someone who has tongue-tie might have difficulty taking out his or her tongue. Tongue-tie can also affect the way a child eats, speaks and swallows. The symptoms are difficulty lifting the tongue to the upper teeth or moving the tongue from side to side, trouble taking out the tongue past the lower front teeth and a tongue that appears notched or heart shaped when stuck out and speech difficulties of speaking certain sounds as the tongue can-not reach the palate. The complications of tongue tie are 1) Breast-feeding problems [4]. Breast-feeding requires a baby to keep his or her tongue over the lower gum while sucking. If unable to move the tongue or keep it in the right position, the baby might chew instead of suck on the nipple. This can cause significant nipple pain and interfere with a baby's ability to get breast milk. Ultimately, poor breast-feeding can lead to inadequate nutrition and failure to thrive. 2: Speech difficulties [5]. Tongue-tie can interfere with the ability to make certain sounds — such as "t", "d", "z", "s", "th", "r" and "l". 3: Poor oral hygiene. For an older child or adult, tongue-tie can make it difficult to sweep food debris from the teeth. This can contribute to tooth decay and inflammation of the gums (gingivitis). Tongue-tie can also lead to the formation of a gap or space between the two bottom front teeth. 4: Challenges with other oral activities. Tongue-tie can interfere with activities such as licking an ice cream cone, licking the lips, kissing or playing a wind instrument. Frenotomy [8] is the standard surgical treatment offered to this congenital anomaly. I describe a new and unique surgical treatment option for this anomaly which is described for the first time in medical literature.
In last 3 years in Jawale Institute of pediatric surgery, I did 21 cases of Tongue Tie release operation (Frenotomy) with methylene blue dye induced infrared laser cutting technique (Group A). 26 patients during same period were put as control (Group B) where the Frenotomy operation was done with conventional technique with electrocautery. Age range was 3 months to 18 years. Maximum follow up was 3 years and minimum of 6 months.
Frenotomy [7,8], is performed conventionally as follows. The child is under general anesthesia and intubated with endobronchial tube. The mouth is opened by mouth gag. The tongue held with Babcock forceps and pulled. The frenulum is cut with cutting type of electrocautery to lengthen the tongue till it comfortably comes out of mouth. Hemostasis is achieved. Any blood and saliva is sucked out immediately to avoid going towards glottis.
The technique of Tongue tie release operation (Frenotomy) by methylene blue dye induced infrared laser is as follows. The child is put under short general anesthesia. The mouth is opened by mouth gag. The tongue held with Babcock forceps and pulled. Methylene blue dye is injected over and into the frenulum till it is well colored with blue. The frenulum is cut with a laser of 950 nm and 20 Watt in power (Photo1). The laser fiber held with laser guide is concentrated on blue dye to cut the tissues. The newly exposed area is irrigated with more drops of Methylene Blue dye and further targeted by the laser. The tongue is released till it comfortably comes out of mouth (Photo2). Hemostasis is achieved. Any blood and saliva is sucked out immediately to avoid going towards glottis. Patient is discharged on same day and asked to follow up after one week (Photo3).
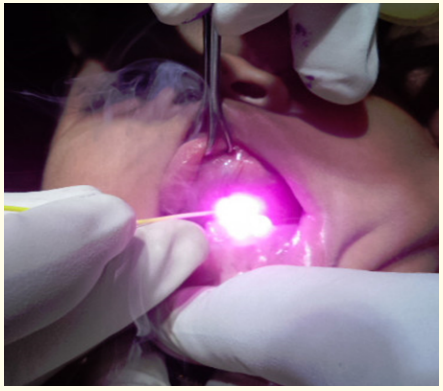
Photo 1: Frenotomy operation by methylene blue dye induced infrared laser cutting.

Photo 2: Frenotomy complete.

Photo 3: Frenotomy after one week.
The laser machine used for this purpose is a 950 nm 20-watt infrared fiber coupled diode laser. The laser diode in the machine produces the laser which is coupled with an optical fiber of 0.1 mm fiber and a wire of 1 mm Jacket. The wire is fixed in a laser guide which is held by the surgeon in his fingers as a pencil to be used it on patient. The cost of the machine is only USD 500.
In group A, 1(4.76%) patient complained difficulty in eating and swallowing, 2 patients (9.52%) had pain postoperatively for more than 48 hours. No patient had edema of tongue. There was no postoperative bleeding. In Group B, 6(23.07%) patients patient complained difficulty in eating and swallowing, 12(46.15%) patients had pain postoperatively for more than 48 hours. 6 (23.07%) patient had edema of tongue and 2(7.69%) patients had mild oozing of blood after 48 hours. Thus, morbidity in laser group was negligible compared to the control group.
Infra-red lasers of 950 nm are cheap and easily available compared to other lasers. Infrared laser of 950 nm has a much better coagulation power compared to electrocautery. Hence the operation is bloodless. Any significant bleeding into the oropharynx can go into glottis and lead to aspiration and serious complications. But the drawback of infrared lasers is that they are effective only against its opposite color. It means infrared laser will be best effective against its opposite color blue and non-effective against pink. If infrared laser is fired on tissues which are pink, a lot of it is reflected and effectiveness is poor. On the contrary, it is very effective against its opposite blue color. Hence, a blue dye has to be infiltrated on pink tissues to make it effective. Methylene blue as a dye that is already FDA approved to be used topically as well as intravenously in human body. Hence there are no ethical issues for using it on human body.
This new and unique surgical treatment option for this anomaly which is described for the first time in medical literature. Although this technique has a vast application in other areas of surgery, this article limits to its use in frenotomy operation. The group A is clearly a winner as it has little morbidity compared to group B. The advantages of this technique over the conventional are as follows. The operation can be performed on a day care basis and can be done under short GA compared to the conventional which requires over night stay as it requires full GA with endobronchial intubation. The operation is blood less as the infrared laser of 950 nm has a much better coagulation power compared to the electrocautery. As the laser is quite precise, the collateral damage produced by laser is much lower compared to electrocautery [9,10]. Because of the Methylene blue dye, a cheap infrared laser (USD 500) can be used for this purpose. Otherwise, a high frequency 2000 nm and high wattage (40 Watt) laser has to be used which is extremely costly (USD 50,000) and is not affordable to most surgeons. Since the only disadvantage of laser against electrocautery was cost which is eliminated in this technique. Hence it is a clear winner over the conventional technique. The technique also becomes a foundation as a learning experience for its wider application in other areas of surgery.
The Tongue tie release operation (Frenotomy) by methylene blue dye induced infrared laser cutting is a safe, effective and affordable technique. The technique can be used on plenty of other operations in surgery.
Acknowledgments: There are no Acknowledgments to be made about this research study.
The first author is the inventor of the technique who has also done the clinical study.
Not applicable.
The first author have done the whole research and study with his own money.
There are no conflict of interests amongst the authors.
Not applicable.
Not applicable.
Copyright: © 2019 Sagar A Jawale. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.