Kannor Patience1*, Adjei Rose2, Ebenezer Kwesi Armah-Ansah3 and Naah Jude4
1Department of Community Medicine, School of Medical Sciences, University of Cape Coast, Ghana
2Department of Education and Promotion, School of Public Health, KNUST, Ghana
3School of Public Health and Psychosocial Studies, Auckland University of Technology
4School of Public Health, UDS, Ghana
*Corresponding Author: Kannor Patience, Department of Community Medicine, School of Medical Sciences, University of Cape Coast, Ghana.
Received: January 29, 2019; Published: March 14, 2019
Citation: Kannor P., et al. “The Role of Geographical Accessibility in the Utilization of Maternal Skilled Services”. Acta Scientific Paediatrics 2.4 (2019):36-42.
A million women continue to die annually from complications of pregnancy or childbirth and many more suffer prolonged or permanent post-partum ill health or disability. Distance to care is known to influence uptake of health services. The purpose of the study was to ascertain the role of geographical accessibility in reducing maternal mortality. This was a qualitative study that was conducted among women who were in their reproductive ages (15-45). With the aid of a semi structured interview guide, 15 women were purposively selected and interviewed for the study. The data were analysed using an inductive content analysis approach.
It was observed generally the high cost of transportation coupled with poor road network and long distance to a health facility deter most women who are in their reproductive ages (15-45 years) and have a child in the study area from accessing the required number of antenatal services as prescribed by WHO. The results revealed that a number of the respondents did not see distance as a barrier in accessing skilled delivery services since they are much particular about the services, they receive rather than the financial constraints. However, respondents indicated the absence of good road network and a health facility in the community makes it difficult to take utilize health facility.
Keywords: Geographical; Health Facility; Women
Pregnancy periods, during delivery, and after delivery periods pose as a high risk to maternal deaths and health and an important danger to the unborn child and the newly delivered child [1]. As a result of the unimaginable increase burden of mortality and disability in women of reproductive age, United Nations (UN) in 2000 among its 189-member states promised to work towards arriving at the set of Millennium Development Goal. Maternal Mortality Ratio which was one of the targets of MDG was reduced by threequarters in the 2015 and much was felt within Sub-Saharan Africa [2].
Safe delivery as an indicator of MDG 5 is an important idea about the effectiveness of the goal. Improvements on this goal (MDG 5) has been quick as there has been reduction in MMR by half between 1990 and 2005. Thus about 230 deaths have been cut off with 290 deaths per 100, 000 live births still remained from 520 to 290 deaths [3].
Although, tremendous efforts had been made by international communities and organization to reduce maternal mortality, but the situation is still high because one-third of a million women still lose their lives from pregnancy related causes annually and even to the extent of developing permanent health conditions such as disability [3,4]. Majority of these problems, about 90%, is suffered by developing nations of Sub-Saharan Africa and South Asia [5].
To reduce maternal mortality, different interventional programmes had been identified and put in place by different countries. Improving access to health care or facility with qualified or well-trained health workers and providing quality midwifery services from efficient midwives and life-saving obstetrics measures at conception is a well-known instrument in reducing maternal mortality [6].
In Ghana, different health interventional programmes have been initiated by the government for the past three decades. In 2003, the Government of Ghana (GoG) introduced the removal of the user fee in order to help maternal mothers have easy access to maternal health services in such a way that finance will not be a burden to access health care and due to its success, it became a nationwide programme in 2005 with free caesarian section to all pregnant women as part of it [7].
The fee exemption policy was stopped in 2005 and within the same year, the Government of Ghana (GoG) operationalized the National Health Insurance Scheme (NHIS) to help curb the situation of cost as a barrier in accessing health care. The policy was not automatic but one needed to be registered on the scheme in order to benefit from it, denial to register will lead to a situation where individual, even pregnant women, will be asked to pay for the cost of health care as opposed to those who are on the scheme and will not pay anything but will be given the same service. In light of this, in the year 2008, Maternal Health Care Program was initiated by the Ministry of Health to take care of the situation of fee paying with respect to maternal mothers. Services that were catered for by the program included: six (6) antenatal care visits, delivery care including care for complication, two (2) post-natal care visits within a 6 weeks’ period after childbirth and care of infants up to 3 months of age [7].
More than a decade now, pregnancy related complications and deaths are still of public health concern and also are global problems. Majority of these deaths occur during delivery and much of it are found or occur in developing countries as compared to developed ones and the gap between the two in terms of maternal mortality ratio is huge [2]. Its deemed necessary to find out other factors aside the time of delivery that can cause an increase in maternal mortality. As a result, this study therefore seeks to ascertain the role of geographical accessibility in reducing maternal mortality in Brenue Akyinim of the Komenda Edina Eguafo Abrem (KEEA) Municipality of Central Region, Ghana.
Notwithstanding the success in reducing MMR by three-quarters by 2015, this has not been the case in Sub-Sahara Africa specifically Ghana. According to the 2010 population and housing census, maternal mortality accounted for 9% of death among women aged 15-54 years in Ghana [8]. The majority of these deaths are seen between those aged 25-29 and this group is very active in terms of child birth, accounting for one-fourth of all birth. 11.3% of all women within their child bearing years (15-49) die as a result of pregnancy related [9].
The MMR at the national level is 485 deaths per 100,000 live births, which is higher than the 2010 WHO estimates of 350 per 100,000 live births and the 2007 GHMS estimates of 378 deaths per 100,000 live births for the 5 years preceding the survey [6,9]. According to the Ghana Statistical Service 2014 report, the maternal mortality ratio of Central Region (520 per 100,000 live births) in 2010 was higher than the national average of 485 per 100,000 live births. In the year 2006, the region recorded 87 maternal deaths (169/100,000).
Despite these, most studies on maternal mortality in Ghana focused on utilization of skilled services [10,11], antenatal care utilization [12,13] or access to care [14]. Major causes of maternal death in other studies which are mostly quantitative in nature have been concentrated on maternal age, educational level, wealth, and other socio-demographic variables [11,15]. Ghana Statistical Service in 2009 and the Ministry of Health in 2011, identified geographical location as cause of maternal mortality in Ghana [6,16]. This study therefore, using a qualitative approach, seeks to ascertain the role of geographical accessibility in reducing maternal mortality in Brenue Akyinim.
The study was conducted in Brenue Akyinim which is one of the populated places in the Komenda Edina Eguafo Abrem (KEEA) Municipality of Central Region, Ghana. The KEEA Municipality is bounded to the south by the Atlantic Ocean, the east by the Cape Coast Metropolis, the north by the Twifo Hemang Lower Denkyira District, and the west by the Mpohor Wassa East District. The Municipality covers an area of 372.45 kilometres square with a population of 144, 705 [8].
Brenue Akyinim is 19 km from the regional capital of Cape Coast and 143 km from the national capital, Accra. It is located at an elevation of 66 meters above sea level and its population amounts to 8, 790. It is perched between latitude 5.067 and longitude -1.417. It is popular known for its beautiful beaches which attracts tourist. Kissi, Ayensudu, Ampani, Bronyibima are some of its neighbouring towns. Farming and fishing are the prominent occupation among people of Brenue Akyinim.
Taking into consideration the nature of the research, mothers in their reproductive age (15-45) who have ever given birth to more than one child and have been living in Brenue Akyinim for more than one year prior to the study were the target population.
A sample of fifteen (15) respondents were used for the study. All the fifteen (15) participants were purposively sampled. Inclusion criteria to select participants were (1) mothers within the reproductive age group 15-45; (2) have more than one child; (3) gave birth to at least one of them whiles living in the community (4) willing to offer consent and participate in audio-taped interview. These criteria were used because it gave the opportunity to select respondents who had knowledge about the topic at hand.
The study employed a semi-structured interview guide. The semi-structured interview guide was divided into two sections, A and B. Section A was used to collect data on the background characteristics of respondents. The background characteristics considered were: age, level of education, marital status, place of residence, employment status, monthly income, and number of children. Section B was used to collect data on the role of geographical accessibility in reducing maternal mortality. The information collected was in line with the objectives of the study.
Pre-test of the research instrument was conducted at Anwanda, a town within the Komenda Edina Eguafo Abirem Municipality. This town was chosen because it has similar characteristics as Brenue Akyinim, the study setting.
A separate file was kept for each participant. All names of participants were replaced with pseudonyms. The audio-taped information was transcribed verbatim and translated from the participant’s local language into English while making reference to the filed notes where necessary. The transcription process helped the researcher to get closer to the data and understand critically what each participant said about their experiences and challenges and how it was said. The analysis was guided by an inductive content analysis approach. Principal themes that emerged from the role of geographical accessibility in reducing maternal mortality were identified by highlighting material in the interview transcripts.
The background characteristics of respondents in the study area are described in Table 1. The results revealed that most (4) of the respondents were aged from 21-25 years, with a number of the respondents (10) with junior high school education. Married (12), farming and trading (6) each while Six each had income above ₵100 and did not know their monthly income.
An antenatal care service is very important to every pregnant woman in order to keep a healthy foetus to term without any complications to both the mother and the child. The geographical location of the services and where the pregnant woman is, serves as a great determinant to its utilization. From the data gathered, some of the emerged themes were, transportation cost, poor road network, and absence of a health centre in the community.
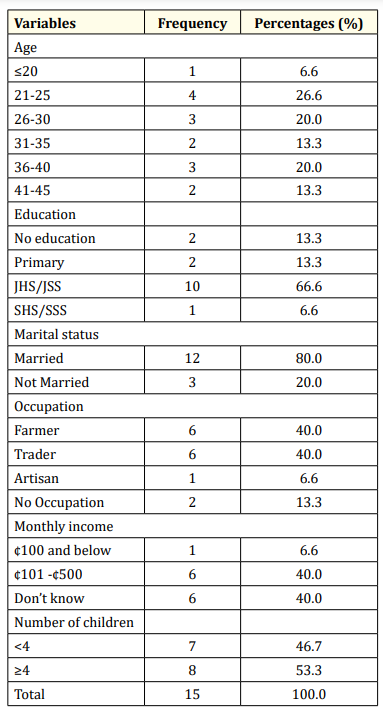
Table 1: Background characteristics of respondents. Source: field work, 2018
The cost of transportation was a major barrier identified by almost all the respondents. The high cost of transportation deters them from accessing health care services such as ANC when pregnant. They identified that, it can cost about gh50 to get a transport to hospital not necessarily for ANC but during emergency. During non-emergency periods, it cost not less than GH 10 to get to a health facility because there is no health facility in the community. The closest one is Kissi or Bronyibima or Elmina which is about one hour from here.
A respondent indicated that;
From here to Ayensudu junction (a community in KEEA) is GH2.50p and from there to Elmina is another GH2.50p. So, in all it will cost GH10. That is when we are going to Elmina. This is a challenge for us. Because of the fare, some will not even go to the hospital throughout the pregnancy period till she gives birth. Those who are able to go are those determined to go. When my time is due to go to the hospital for check-up, I have to fast and save some money before I can go.
Another respondent indicated that, she only goes to the hospital when pregnant because she always has problem during pregnancy. If not for that reason she wouldn't have mostly attend Antenatal services.
For those of us who go to Cape Coast Teaching Hospital, it cost us about gh20.00. For me because I have problem with my pregnancy, anytime they ask me to come to the hospital I have to find money and go. If not for that I don't think I would go there as I am doing now.
For one of the respondents, her frequency of visit to the hospital is influenced by the transportation fare not the number of times she is been told by the health worker to visit the health centre.
eeeeiiii.......no, if the doctor asks me to come may be three times a week, I will only go there once because the transportation fare is costly.
Regarding the poor road network, respondents identified that due to the poor road network they mostly feel pains on their way to the hospital and for some instances if care is not taken, they believe that they can gave a miscarriage.
The road is not good. Recently, I was close to eight months pregnant and I took a taxi to Ayesundu, due to the potholes I nearly gave birth in the car (laughs).... I felt pains all along. The road is really not good for us. We suffer a lot, especially us (pregnant women) when using it.
Regarding the absence of a health centre and distance a respondent indicated that, the absence of a health facility in the community and the distance to the closest one makes some of them feel reluctant to go far to access maternal health services. Respondents identified that they can spend about an hour from their town to the nearest health facility, thus, Elmina or Kissi.
There used to be a hospital here but it’s been taking to the next town. It is not that we sometimes don't want to go but we are busy with farm work so if there was to be one, we will just pass by since its close as compared to going far away. From here to Elmina, we spend about one hour on the road. So, you see, if we have one here it will help us a lot.
The use of skilled delivery services is really important for maternal mothers during delivery. From the responses, it was realized that some of the respondents gave birth at a health facility whiles other also delivered at home. Different reasons were given by each group of people (those delivering at a health centre and those who deliver at home).
With regards to those who delivered at home, the major reason was fear of complication and difficulty during delivery. They explained that health centres have the necessary equipment which help prevent any complication in case there is any as compared to home delivering where if there is a problem you might die or be taken to a health facility. So, they will rather prefer you go to the health facility to deliver.
I have not given birth at home because I am afraid. If there is any problem those attending to you at home cannot take care of it but in the hospital, you will be provided with the necessary care.
I gave birth to all my children at the hospital. With the exception of one whom I delivered on my way to the hospital but even for that I went to the hospital. I go there because I suffer before I can give birth and after giving birth I bleed a lot.
Another respondent said this;
The pregnancy was difficult so they have to operate me
Some also go to the hospital based on their previous birth experience and advice from health care providers.
I had one miscarriage so the nurse advised me to always go to the hospital when I am to deliver
Another respondent corroborated by saying:
I have once given birth to a child about 15 years ago and the child died. For that I did not even go to the hospital throughout the pregnancy. So the nurses told me it is because I did not go to the hospital and I have learnt my lesson from that.
Financial constraint was seen as one of the reasons some of the respondents deliver at home or do not patronize skilled delivery services.
At that moment there was no money. There was no money to be used as transportation fees. I have to take the taxi alone and it will cost me GH 50.00 which I did not have that time
Another reason given was misconception about hospital delivery. A respondent identified that, she has never delivered at the hospital because of what she had heard about hospital delivery. She went further to say that some are beaten with sticks at some hospitals.
The reason why I did not go to the hospital is because of what I heard about you been beaten with stick before you give birth. So because of that I was afraid to give birth at the hospital. I gave birth to all the four at home.
A respondent also indicated that it wasn't her intention to deliver at home. She indicated that by the time she realized it was time for her to go to the hospital it was too late so she delivered at home.
I gave birth to them in the house (laughs).... because at that point I wanted to give birth....it was too late to go to the hospital. I even went to the hospital that day but the nurses did not know my time was up. As I returned home in the afternoon I started feeling the child is coming so I gave birth”.
Respondents indicated a lot of measures that should be put in place in order to reduce their burden or the problems they go through before they deliver. Proximity of the health facility, and good road network were the two measures respondents thought it is appropriate for authorities to put in place in order to reduce maternal problems.
Regarding proximity of a health centre, respondents indicated that they want a clinic or hospital in the community to help ease their suffering of always going far away to attend health care whenever one is pregnant. One respondent said:
For this place we need hospital. Because there is no hospital here we are suffering. Anytime you become pregnant you must go elsewhere to attend hospital which won't cost you less than GH 10.00”.
Another respondent had this to say:
We need at least a clinic here to help us to attend the weekly and monthly services maternal mothers are supposed to go. That will help us save money so that when it is time for us to deliver, we can go to Elmina hospital to deliver (40 years).
Good road network was one of the concerns raised by respondents and they see that as one of the measures to help reduce the health problem of the community. Some of the respondents identified that due to the poor road, they pay fares which they are not to pay. Others also indicated that unwillingness of drivers to travel in the night due to the nature of the road, and others asserted that people even die on the road when they are being taking to the hospital. Their worries were summarized below in these quotes;
Our road....it really disturbs us well. Because of it poor nature the drivers mostly increase the transport fare saying the distance is too far. We are not supposed to pay Gh2.50p but because of the poor road they don't go by what the government transport fares”.
Another respondent said;
The road...even if you have money, not all drivers will go in the night because they say it is dangerous.
Another respondent corroborated that;
Let’s put the pregnant women issue aside. People die a lot in this town because of the road. Before a car will get to town to convey the sick to the hospital, it will be too late and the person will die in the car. Similar thing happened to my in-law.
Aside the respondents craving for these policy interventions, authorities have trained some of the maternal mothers to educate their fellow women about maternity issues and also to take up maternal services. This was done to help those who are unable to attend maternal services to have knowledge about pregnancy related issues. A respondent who is a member of the group said this;
…. we have a pregnancy school at Bronyibima of which I am a member. They make me educate my fellow women to go to the hospital. We also brought some midwives to Ampaem which is closer so that those who don't have money to go the hospital go there.
The study revealed that generally cost of transportation to a healthy facility is a major barrier to women’s utilization of antenatal care in this study. The high cost of transportation deterred most women from accessing antenatal services and this made the women not to attend ANC as recommended the WHO. This is consistent with Mrisho., et al. [17] study on factors affecting home delivery in rural Tanzania which found that although ANC services are available, but women initiate late because of lack of money to continue attendance. Similarly, in a study by Abosse., et al. (2010) in Nigeria, cost of transportation to health facilities was found out to play an important role as a factor adding to non-access to maternal health care. Also, Nyathi., et al. [18] in investigating the accessibility factors that influence antenatalcare services utilization in Mangwe District of Zimbabwe identified high cost of transportation as a barrier among the respondents.
A number of the study respondents revealed that poor road network was another barrier in accessing ANC. The issue of them feeling pains when using the road makes it uncomfortable to use the road frequently. A recent study conducted in Zimbabwe by Nyathi., et al. [18] confirms that uncomfortable transport, poor road conditions and difficulties in crossing big rivers were barriers that most women face in their quest to utilize ANC services Mrisho., et al. [17] also confirms that respondents that women are challenged with poor road network in accessing ANC.
The distance to a health facility due to the absence of a health facility in the community also served as a barrier to the pregnant women. The study indicated that the absence of a health facility in the community has burdened their desire to visit and use ANC since they have to travel long distance of about almost an hour to access a health facility. They travel a distance of more than 10km to the nearest town for health care or more than 20km to the regional capital for health service. Studies from Kitui., et al. [15] and Magadi and Madise [19,20] have shown that distance more than 2km serve as a barrier to ANC utilization. In contrast, Van Eijk [21] indicated that distance was a barrier for facility delivery but not for ANC attendance. Asundep., et al. [12] also contrasted the idea that distance to a facility deters individuals from accessing health care.
With regards to geographical accessibility and mothers use of skilled delivery services, a number of the respondents did not see distance as a barrier to them to access skilled services during delivery rather respondents were concerned of their life or the quality of care they will get at the place they sought for services. This do not conform with a study conducted by Kumar., et al. [22] in India which found out that distance plays an important part in individual’s decision to seek health care delivery services or not to seek those services but deliver at home. Similar observations were made by other studies with respect to distance been a barrier to institutional delivery [21,23]. However, a study by Asundep., et al. [12] in Ghana indicated that it was rather quality of impact that might encourage individual to travel far for health care but not that distance is really the problem.
Generally, respondents stated that financial constraints and fast progression of labour are the major reasons that made some of the respondents to deliver at home. They indicated money for transportation and unaware of labour soon influence their choice to give birth at home. This finding is consistent with a study by Van Eijk [21] in Kenya which found out in that, observed contribution factors to home delivery included the fast progression of labour, difficulty of travel and finance (cost). Thus, most often women realize it’s too late for them to go to the hospital to seek care because their labor is fast progressing and they might give birth on the way to the hospital, and as a result of this, they turn to deliver at home. This factor is mostly coupled with financial problems.
Regarding measures to reduce maternal mortality as a result of geographical accessibility, the findings of this study is in line with findings by Peters., et al. [24] in investigating poverty and access to health care in developing countries. This study revealed that the absence of good motorable road network within the community makes it difficult for pregnant women to take up health care services. The respondents indicated that they feel a lot of pain when using the road and this makes it uneasy for them to use the road regularly when pregnant.
A presence of a health facility in the community was identified by respondents as a measure to help improve their health as maternal mothers and reduce their risk to pregnancy related complications. Johnson., et al. (2011) and Grzybowski., et al. (2011) revealed that issue of proximity to and availability of a health facility improves access to maternal care and a high probability of improved maternal outcomes.
The study revealed that generally the high cost of transportation coupled with poor road network, long distance to a health facility as well as deterred most women from accessing antenatal services and this made the women not to attend ANC as recommended the WHO.
A number of the respondents did not see distance as a barrier to them to access skilled services during delivery since they are much particular about the services they are after rather the financial constraints and fast progression of labour are the major reasons that made some of the respondents to deliver at home.
Respondents indicated the absence of good road network and a health facility in the community makes it difficult to take utilize health facility.
Copyright: © 2019 Sangita D Kamath., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.