Amith Adyanthaya1*, Soniya Adyanthaya2, Prathyusha P3, Ann Meera Johnson4, Afroza KK4 and Lasna MT4
1Professor, Department of Pediatric and Preventive Dentistry, KMCT Dental College, KUHS, Kerala, India
2Reader, Department of Oral Pathology, Yenepoya dental college, Yenepoya University, Karnataka, India
3Professor and HOD, Department of Pediatric and Preventive Dentistry, KMCT Dental College, KUHS, Kerala, India
4Post Graduate Student, Department of Pediatric and Preventive Dentistry, KMCT Dental College, KUHS, Kerala, India
*Corresponding Author: Professor, Department of Pediatric and Preventive Dentistry, KMCT Dental College, KUHS, Kerala, India.
Received: January 28, 2019; Published: March 05, 2019
Citation: Amith Adyanthaya., et al. “Cone Beam Computed Tomography - See the Unseen: A Case Report”. Acta Scientific Paediatrics 2.4 (2019): 15-19.
Conventional radiographs are being used for routine investigations in the diagnosis of intra oral lesions. However with the introduction of CBCT in dentistry, the interpretation and diagnosis of intra oral radiology is being revolutionarized. Here with, is a case report of a 12yr old child with delayed eruption of the 31,32 with the provisional diagnosis of complex odontome confirmed with IOPA and RVG. A detailed history and intra oral examination including palpation and timely interdisciplinary approach with oral radiology, a CBCT scan was performed. A final radiological and histopathological diagnosis of complex odontome associated with dentigerous cyst was established. The treatment of choice was the surgical excision of the lesion along with the teeth associated followed by prosthetic rehabilitation. As a pedodontist, role of interdisciplinary dentistry proves to be a boon in diagnosing various intra oral lesions and planning an appropriate treatment plan for the child.
Keywords: CBCT, Dentigerous Cyst; Odontome; Odontome on Dentigerous Cyst; Odontogenic Lesions
Dentistry has witnessed tremendous advances in all its branches over the past three decades. With these advances, the need for more precise diagnostic tools, specially imaging methods, have become mandatory [1]. Imaging is the most important and most frequently used diagnostictool in dentistry [2]. From the simple intra-oral periapical X-rays, to advanced imaging techniques like computed tomography, cone-beam computed tomography, magnetic resonance imaging and ultrasound have also found place in modern dentistry. Cone-beam computed tomography (CBCT) is a new diagnostic tool that has revolutionized diagnosis and treatment planning in the dental field [3]. Advantages of CBCT includes X ray beam reduction, image accuracy, rapid scan time, reduced dose of radiation and reduced image artifacts [4]. The three-dimensional imaging has made the complex cranio-facial structures more accessible for examination and early and accurate diagnosis of deep seated lesions.
This imaging modality is capable of providing sub-millimeter resolution (2 line pair/mm) image of higher diagnostic quality with shorter scanning times (~60 s). Radiation exposure dose from CBCT is 10 times less than from conventional CT scans during maxillo facial exposure and also it has got great dimensional accuracy (only about 2% magnification) [5].
Odontogenic lesions are common pathologies encountered in the jaw. Dentigerous cyst can be defined as an odontogenic cyst that surrounds the crown of an impacted tooth; caused by fluid accumulation between the reduced enamel epithelium and the enamel surface, resulting in a cyst in which the crown is located within the lumen [6]. From a clinical point of view, dentigerous cysts are generally asymptomatic, slow-growing, associated with the crown of an impacted or unerupted permanent tooth, and characterized by retarded eruption of the tooth. However they may grow large enough to cause destruction of the cortical bone, resulting in fluctuation, spontaneous pain, exudation, and rapid development of the pathology, which are signs of acute inflammation round the margins of the cyst [7].
The Odontoma is a ectomesenchymal tumor of unknown origin, may be related to the presence of impacted teeth, trauma, local infection and dentigerous cysts. Odontoma is most prevalent in the jaws, representing 70% of odontogenic tumors found, which are more considered developmental malformations (harmatomas) than benign neoplasms. Occasionally, the dentigerous cyst is associated with impacted teeth or odontoma. Its association with odontoma is seen in 27.6% of cases [8]
This article aims to report a clinical case with diagnosis of complex odontoma when investigated with advanced radio imaging i.e with CBCT simultaneous lesions with cyst were confirmed and mode of the treatment was planned accordingly.
A 12 year old boy came to the OPD with a chief complaint of swelling and missing lower front teeth. Initially, swelling was small in size and gradually grew to present size. Swelling was asymptomatic and no history of trauma was associated with it. History revealed that the patient had already undergone surgical removal of a lesion assuming it to be a Compound Odontome in the same region 3 years back after the diagnosis made based on IOPA and RVG. On further history taking, it was revealed that the patient had also undergone surgical removal of mesiodens in the 11 region.
No relevant medical or family history was contributory. On examination, all vital signs were within normal limits. Intraoral examination revealed a solitary diffuse swelling on the anterior mandibular teeth region extending from mesial aspect of 41 to mesial aspect of 33, roughly oval in shape measuring about 2cm in greatest dimension. The color of overlying mucosa was normal. On palpation, all inspectory findings were confirmed and swelling was firm in consistency and non-tender.
On hard tissue examination, there were clinically missing 31 and 322 (Figure 1). Intraoral periapical radiograph was advised. On radiograph, an ill-defined radio opaque mass was seen extending from the mesial aspect of 41 to 33. It also revealed the presence of mandibular permanent incisors, 31 and 32. Findings were suggestive of Odontome.

Figure 1: Intra oral photograph showing missing 31 and 32.

Figure 2: IOPA suggests the presence of an Odontome.
Considering patients history of having removed the odontome 3 years back and delay in eruption of teeth after which child reported with mild swelling in the anterior region. Assessing this clinical presentation, patient was advised for CBCT.
The principal feature of CBCT is that multiple planar projections are acquired by rotational scan to produce a volumetric dataset from which inter relational images can be generated.
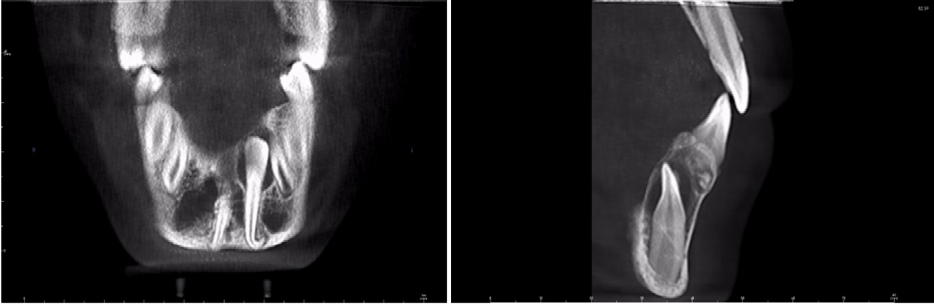
Figure 3: Radiolucent lesion in the mandibular anterior region involving the crown of 31 and 32.

Figure 4: Shows positions of impacted 31 and 32 within bone, their relationship to the calcified structure, Superio Inferiorly and to the roots of adjacent teeth with dilaceration of the same.

Figure 5: Shows position of 31&32 and their relationship to the calcified structure superior inferiorly along with intact cortical border of mandible.

Figure 6: Shows position of 31 and its relationship to the calcified structure labio-lingually, along with increased follicular and development of a cyst.
Considering the various clinical, radiological and CBCT, following Differential Diagnosis was made:
The diagnostic hypothesis based on the clinical, and imaging examinations was of a Complex odontome with dentigerous cyst.
In the present case, the radiolucency surrounding the extent of the calcified structures and the extent of the radiolucency beyond the crown of the involved teeth and the dilacerations of the roots were totally missed in IOPA and RVG. Hence the, CBCT played a vital tool in seeing the unseen.
Following an inter disciplinary approach, the following treatment plan was be considered:
The surgical procedure was performed under local anesthesia. A linear and scalloped incision was performed, flap detachment, and osteotomy to expose the odotome and cystic lesion (Figure 7). First the complex odontome, and then the impacted teeth with cystic membrane with all its extension were removed followed by bone curettage (Figure 8,9) of the surgical bed, hemostasis and sutured.

Figure 7: Incision, flap detachment and osteotomy to expose the lesion.

Figure 8: Removal of impacted teeth and the cystic lesion.

Figure 9: Surgically removed incisors with the cyst.
Postoperative recommendations, pharmacological therapy and clinical control visits were prescribed. Tissue samples were sent in 10% formalin for histopathological study (Figure 10).

Figure 10: Tissues in 10% formalin sent for histopathological study.
The resulting anatomo and histo-pathological report (Figure 11) described an odontogenic lesion, characterized by a proliferation of well-defined tissue structures consisting of deposits of enamel and dentin, surrounded by fibro-connective tissue. The findings corresponded to a complex odontome with cystic changes related to a dentigerous cyst.

Figure 11: Eosinophilic stained material with a dentin like structure
Odontomas are non-aggressive hamartomatous developmental malformations or lesions of odontogenic origin of unknown aetiology. They often remain asymptomatic and undiscovered until revealed by routine radiography [9].
Cases of simultaneous pathologies are rare, especially of a complex odontome related to a dentigerous cyst. An important consideration is that the diagnosis based only on radiological appearance of these lesions is a challenge for the dentist, as these lesions do not possess many defining clinical and radiographic characteristics.
Qizhang., et al., Astekar., et al. reported cases of a complex odontoma with a dentigerous cyst, confirming the relationship between odontomas and cysts with tumors of odontogenic origin. Due to their large size, odontomas can affect neighboring structures such as the roots of teeth [10,11].
Dagrus., et al. reported a case of a dentigerous cyst arising from a large complex odontoma, located in the right posterior region of the jaw. They reported there were no clinical signs of inflammation, but there was the absence of molars and mild pain in the affected area. Their findings were in accordance with our present case describing the case of a complex odontoma associated with a dentigerous cyst in the anterior mandibular region. However, there is disagreement regarding the description of symptoms, as in the present case, the child did not complain of pain. These differences could be explained by the size of the lesion and the degree of involvement of the mandibular canal [9].
Simultaneous lesions are rare and the diagnosis based solely on the radiographic appearance poses a great challenge to dentists. For this reason when in doubt it is important to carry out advanced radiographic investigations like CBCT. These definitely help in identifying radiographic characteristics of the lesion and contribute to the understanding of a correlation with surrounding structures.
In present case, this type of lesion does not present clear and conclusive characteristics with routine X-ray and RVG, then it becomes mandatory to include panoramic images and three-dimensional imaging modalities like CBCT [12].
Conventional methods for the evaluation of the lesions of the maxillofacial complex are often inconclusive providing the need for an additional advanced radiographic method. This case report describes the of role CBCT as an important diagnostic tool since it provided images of the lesion in all planes and thus enabled the localization, extension and internal structure of it thereby aiding in the final diagnosis and accurate treatment planning.
None.
Copyright: © 2019 Sangita D Kamath., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.