Sam Hassan1* and Rowell Sinlao2
1
Associate Professor of Paediatric Medicine, Department of Paediatrics, Mediclinic City Hospital Dubai, United Arab Emirates
2
Paediatric Nurse, Department of Paediatrics, Mediclinic City Hospital Dubai, United Arab Emirates
*Corresponding Author: Sam Hassan, Associate Professor of Paediatric Medicine, Department of Paediatrics, Mediclinic City Hospital Dubai, United Arab Emirates.
Received: February 4, 2019; Published: February 08, 2019
Citation: Sam Hassan and Rowell Sinlao. “Electronic Emails Communication with Patients in A Busy Pediatric Practice: Four Years Prospective Study and Literature Review”. Acta Scientific Paediatrics 2.3 (2019):03-11.
Purpose: to study the use of electronic email as a communication tool augmenting the traditional consultations and assess in details topics and concerns raised by parents’ emails.
Methods: prospective descriptive study for 4 years in a busy pediatric practice.
Results: a total of 4155 emails received between January 2015 – December 2018, 2275 emails by the consultant and 1880 by the nurse. Reorganization of the email communication reverse the ratio between the nurse and the doctor after first two years assessment (Figures 3 and 5). Topics and concerns raised by emails were variables (figure 4, table 1 and table 3). Some concerns were included as attachments (table 3 and figure 6). There was no restriction for writing email by parents wherever they are in different countries. Detail classification of the emails enabled the service to develop better communication during consultation and written information by identifying the gaps and expanding the service outside the boundaries of the wall of clinics. There were no single risk of breaching privacy and parents were happy using this way of communicating.
Conclusion: Emails offer augmenting way of communication that moves the service from episodic traditional consultations into continuous care wherever the patients are. It is convenient, time saving, less costly, provide flexibility, written information, trail, wide accessibility, and build trust with patients. Emails are storable and can be used to assess topics raised by patients to improve communication and services.
Keywords: Communication; Paediatric; Children; Emails; Healthcare
Communication is a corner stone factor in delivering adequate healthcare to any community. Poor communication with patients or their careers results in serious consequences that may include medical errors, management plan failures, events harms, social disadvantages, physical impacts, emotional and psychological harms. Failure of communications represent the commonest theme in formal complaints in the health systems worldwide. For example, in the UK where there is a National Health Service (NHS), poor communications fuels rise in NHS complaints [1]. According to the Parliamentary and Health Service Ombudsman, England’s hospitals top listed cause for complaints remains the same over years, is poor communications [2]. The UK General Medical Council consider communication with patients as a fundamental part of the Good Medical Practice not only with patients but their relatives, and with colleagues in an honest, sympathetic, supportive and taking in account the diversity of patients believes and language [3]. Despite the importance of communication, there are little guidance reported in literature about the effective ways to achieve successful communication with patients in particular the use of electronic email communication. On the other hand, in a busty to busy environment whether in primary or secondary settings there are always diversity of daily busy tasks leading to immense demands that will make clinicians and nurses to forget to improve communications despite current calls to pay more attentions towards communication improvements right from the Medical Schools teaching [4].
Communication is different from information giving. It is a two-way balance between listening and talking (Figure 1). Stephen Covey in his book “The seven habits of highly effective people” wrote; “40% of our waking time spent in listening yet we are never really taught how to listen” [5]. Listening is different from hearing. You can listen to someone by reading their emails but not always engaged with them while hearing them. To really engage with someone like your patients you must first seek to understand them before you make yourself understood. Only by this way clinicians can succeed to achieve empathy with their patients which is the most important first product of communication. Empathy is understanding the others from their point of view by listening not only to what they say but what they are unable to reveal. Patients can easily detect when the clinicians are not engaged with them in a meaningful way or they are distracted and email communication not different as it is a reciprocal communication too. There are 3 elements in traditional way of communications (face to face consultation). The spoken words represent only 7%, the voice and tone 38% while the most important aspect of communication is the body language which represent 55%. In medicine for hundreds of years the main way of communication was this traditional way of face to face consultation. More recently, other ways of communications in medical practice emerged and augmented the traditional consultations. For long time patients feels their needs are unmet by the traditional face to face consultations. In a survey published in the British Journal of Hospital Medicine 1989, patients feel that their needs were unmet due to poor communication, lack of time, difficult to remember, and stress lead to poor information retain [6]. Having an email at their own pace allowing patients to ask questions and help them to understand better other than the misleading information they may get from internet which is largely unregulated resource of information that potentially mislead [7] Email communications with their health providers reduce that confusion resulted from internet and extend care to their homes. Widespread use of emails by people and services started 20 years after the first email programmed and sent by Ray Tomlinson in 1971. Now the use of emails revolutionised many industries, customer services and government departments yet in the healthcare services it is underutilized and many hospitals and primary care centres are still mainly using letter typing and traditional communication with their patients which are cost and time consuming. Healthcare professionals are among the last not to use emails with their clients. There are recommendations by many healthcare advisory groups in many countries such as the Committee on Quality of Health Care in America to shift from the episodic care of visits and traditional appointments to a continuous process of communication and care. They advised that electronic communications such as emails can help in achieving this goal [8] In fact using electronic communication is more than adding something onto the traditional practice. It is about re-engineering practice to enhance accessibility. Email is a valuable communication tool, makes doctors more accessible, represent thorough exchange of information and continuity of care. Medico-legally emails stand more than phone calls, they are copy-able, redistributable, trailing, storable, reviewable, more efficient, auditable and researchable to gain insight and improve practice. Likewise, emails are documented consultation activity that maybe reimbursed easier than calls, in fact many insurances in the USA pay for email activities. Email communications in pediatrics as any other field of medical and surgical practices may offer learning process for clinicians, nurses and other professionals to the in site and the daily needs of their care. It provides classifications approach to the needs of parents and patients and enable clinicians to widen their knowledge accordingly. In this prospective study of email communication with parents we provide such approach and classification for first time. To our best search this is the first research of its kind in English medical literature. Such type of study will help to improve our communication based on a patient-centered care beyond boundaries of medical practices and by classifying and studying their continuous concerns beyond the boundaries of health centers.

Figure 1: Communication balance.
This is a prospective descriptive study about electronic communication namely emails with parents or careers of children seen in inpatients and outpatient consultant practice in a busy teaching hospital. The service offers consultations of all modalities of care from primary to secondary or tertiary services. The consultations are booked before or sometimes on the same day as a 30 minute for each new patient or less for reviews. Longer times may be needed for certain cases by the discretion of the consultant. Patients advised to arrive 20 minutes before appointment time to allow time for registrations and vital and anthropometric data taken by the nurse. Each patient got a file in the Hospital Information System (HIS) which included all consultations and a contact information for at least two telephones and an email. All results, prescriptions, and ordering investigations are electronically prepared. Parents so often required to communicate with us by telephone but they have to come through a busy switchboard system and the consultant may be busy while the nurse cannot answer the parents query. Some parents wanted to send reports or pictures that only sendable by emails. On the other hand, the results of the investigations were informed and discussed with the parents before this study by telephone calls which are so often takes long time, busy lines, auto replies, telephone switched off or outside range. Moreover, telephone calls are not copy-able. We therefore decided to use emails to communicate with parents and when we achieved good results decided to do a prospective study of it. Following the consultation, the patients were encouraged to email us about their concerns and a secure hospital email of the consultant was provided. Later on, both the nurse and the consultant emails were given. If investigations are awaited we take at least one email from the parents or both parents and kept in a secure place in a book for the purpose with the label of the patient as well as in the HIS system. For this prospective study, once an email received a copy was made and stored securely in the hospital hard drive. Emails copied under their time and date per months and years and classified according to the concern or topic raised in them before storage. Following completion of 12 months of the year emails were sorted according to their topics or concerns and then categorized according to the systems or conditions raised. Some emails got attachments of pictures, audio or reports and these were categorized depending on the concern raised and the attachment. Responses to the emails were not included in this study. Mobiles and other than the hospital internet computers were not used to access patients emails or reply to them. Patients verbally informed about sharing with them communication by their emails for results and other related issues. When they emailed us, we ask them to confirm that using the same email for communication is acceptable. When the doctor is on leave or weekend and public holiday we send autoreply stating when the parents should expect an early reply and on the same autoreply we provide extension to be called in cases of emergency or urgent need. During the working days when we receive an email either reply sent immediate on the same time the email accessed or if busy we inform parents about when to expect a reply. The parents email first read thoroughly so as if we find that the condition need immediate clinical review or emergency check we advises parents accordingly for the child to be reviewed in clinic or to be taken to the Emergency Department. However almost all the concerns raised are of non-urgent nature to need emergency but quite few of them we arranged follow up appointment in one to two-day time.
A total of 4155 emails were received between January 2015 and December 2018 from parents attending our consultation practice in one clinic in Mediclinic Teaching City Hospital which is a teaching hospital for Mohammad Bin Rashid University of Medicine and Health Sciences. The consultant received directly 2275 emails while the nurse direct emails were 1880 quite few of them copied to the consultant too. The practice providing primary, secondary and tertiary service for children below 16 years of age. Figure 2 shows the total number of emails on a monthly basis and figure 3 shows the total emails in each year for the consultant. It was noted that the number of emails to the consultant decreased despite the total number of patients increase over the years. This is likely due to several factors one of them is related to this study when after first 2 years we assessed our results and presenting them allowing us to reengineer our communication. After this mid-study evaluation, we identified areas that needs improvement of communication with parents before they leave the consultation, providing written and verbal information about them, and providing the nurse email to deal with some concerns related to appointment and filtering others as needed hence the email ratios reversed between doctor and nurse. We classified the emails based on parents’ concerns as shown in figure 4. This allows us to identify areas of communication that need improvements which was done verbally during the consultations and by providing written information such as about vaccinations, nasal congestion, colic, feeding problems, eating disorders, management of fever at home, G6PD, weaning, eating problems, sleep problems, UTI, and others. The nurse email was initially not shared with parents but following the midterm assessment we provided both emails to the parents hence more of parents emails about different issues goes to the nurse Table 2 and Figure 5. Following the use of written information and enhancement of communication during the consultation it has been found that parents less likely need to come back to us by emails. The topics that parents raised in their emails are as listed in table 1 and figure 5
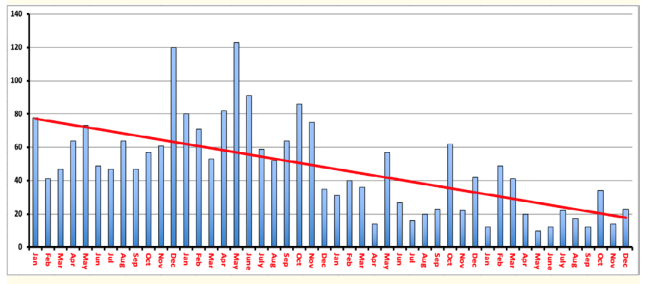
Figure 2: Total number of emails to the consultant each month for 4 years 2015 – 2018.
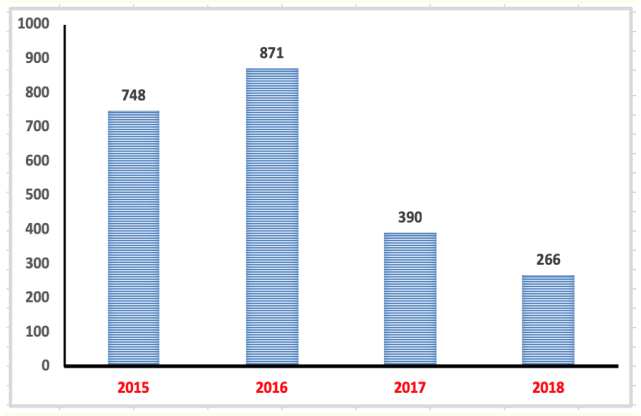
Figure 3: Total number of parents emails to the consultant each year 2015 – 2018.
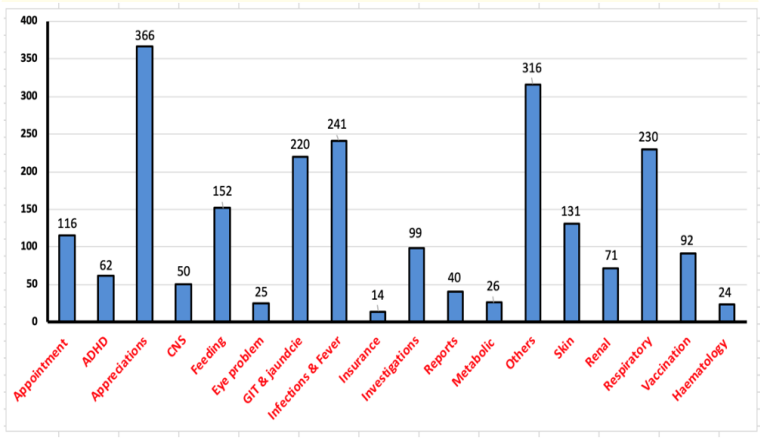
Figure 4: Types of emails received classified according to parents concerns 2015 – 2018.
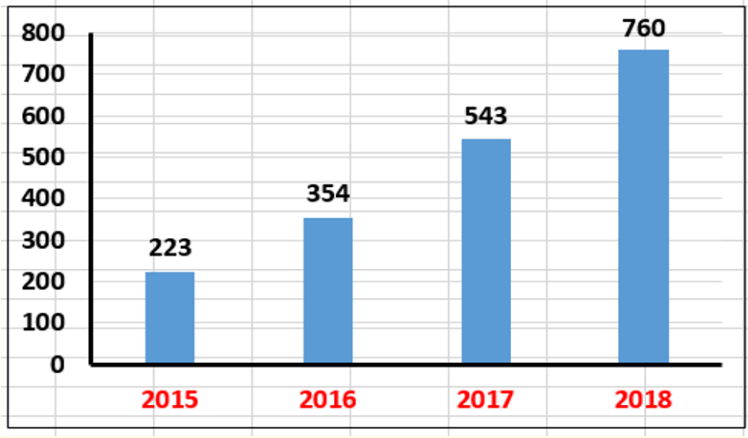
Figure 5: Total number of parents emails to the nurse each year 2015 – 2018.
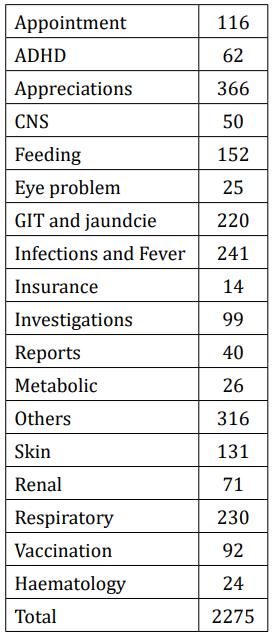
Table 1: Types of parents emails according to the concerns raised in 4 years 2015 – 2018.
It is clearly noted from table 1 and figure 4 that the commonest concerns making the parents to seek an advice or appointment are fever, respiratory infections, gastrointestinal problems, skin rashes, appointments and appreciations. In the last two years 2017 and 2018 concerns about appointments were more tackled by the nurse as well as communicating the results after filtered by the consultant when clear instruction can be done by the nurse. More complicated results communicated direct to parents by consultant. Conditions that listed in table 3 were indiscriminately shared by the doctor and the nurse in the first two years of study (2015 and 2016) while were more organised in the next two years 2017 and 2018 as in table 2.
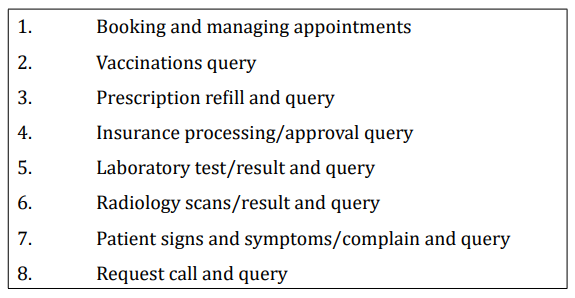
Table 2: Aspects making nurse involvement in parent’s emails increased.
Interestingly more than 7% (n= 174) of the emails received from parents had attachments. Table 3 and Figure 6 showed the type of emails with attachments. It is clearly the comments cause of concerns is skin rashes mostly of viral origin however cases of Scarlet fever, impetigo, eczema, bruises, and other skin manifestations were included. Interestingly other recurrent concerns with attachments were the outcome of the BCG vaccinations scar, eye infections including sticky eye resulted from nasolacrimal duct stagnation, medications, and miscellaneous issues listed under others and in Table 4. Such classifications and retrospective analysis of the emails allowed us to identify the areas that we need to provide more information during the face to face consultation and providing written information.

Table 3: Emails with attachment.
Table 3: Emails with miscellaneous concerns.
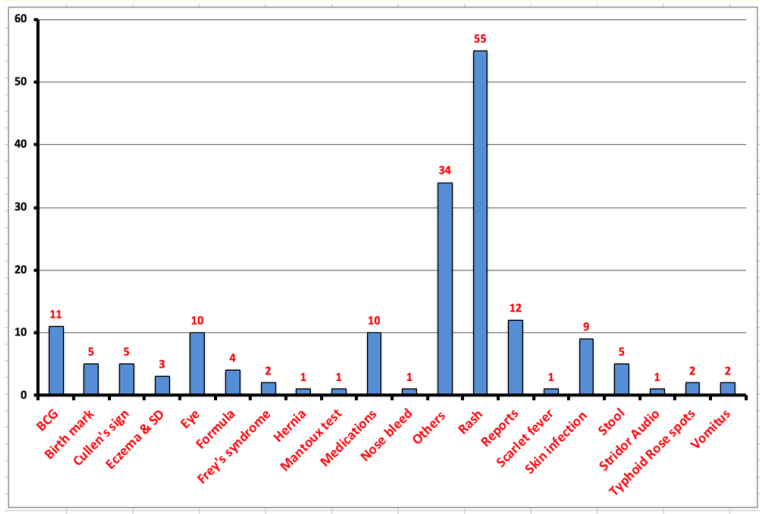
Figure 6: Types of attachments received with parents’ emails communications 2015 – 2018.
It is very important to note that parents can easily use the email communication even when they are outside the country for a holiday or back to their mother country for a break. In table 4 and figure 7 are number of emails received from parents about different issues and concerns related to their children while they are away. About 6% (n = 132) of the emails received from different countries. The figures may reflect expatriate numbers or from neighbouring countries. Interestingly the highest number of emails received from the UK, Oman and Saudi Arabia. Most of these emails parents seeking advises of what to do or prescription repeat.
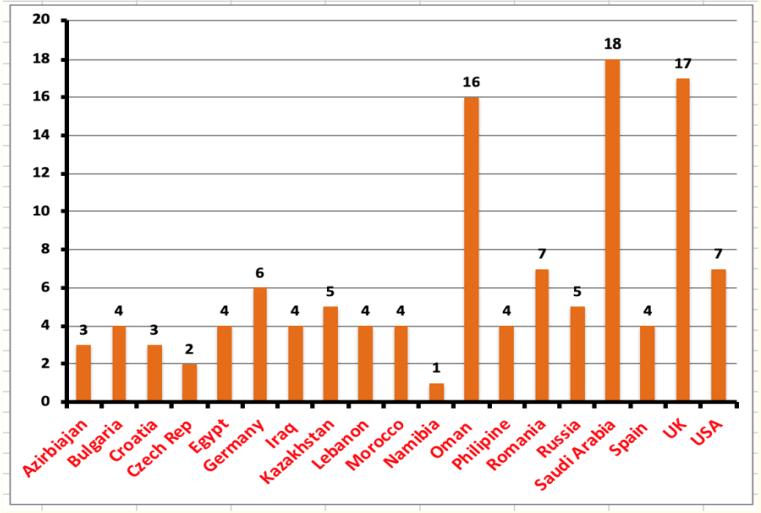
Figure 7: 6% of parents emails received while in other countries 2015 – 2018.
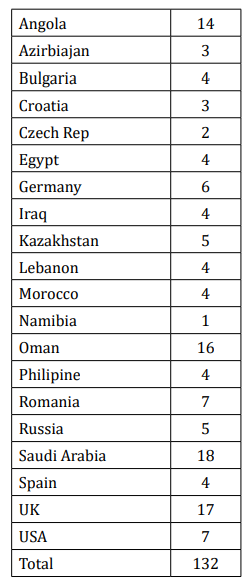
Table 4: Parents emails received while they are outside the country.
It has been noticed in the last few years that increasing number of clinicians and patients turning up to the internet to use emails for communications about patient care from home [9] however, detail assessment of parents’ concerns in their emails with their paediatricians have not been fully reported. In this descriptive prospective study parents’ concerns in their email to paediatrician in one busy practice were analysed in details for 4 years. Emails were assessed day by day in each month for 4 years. Emails were classified according to the concerns raised and farther classified for the attachments used and the country of origin where the emails were issued. This classification is quite useful to evaluate topics and concerns raised by the parents and action taken to improve communications throughout the patients’ care.
Proper and effective communication particularly its listening part is one of the most important skills that health professionals needed so as to get interpersonal relationships, understand others, and build trust with their patients’. In fact, some sort of communications exists in all living species to be able to function effectively. Mankind supposed to have the most complex communication among other Earth species. During illnesses, human communication is so important and should take more empathy than before. Communication by writing developed long time ago about more than 5000 years ago in the Southern Mesopotamia which is called Sumer by the invention of the Cuneiform writing. Clay tablets used to spread Medical and other knowledge from Sumer to other parts of the world at the time [10,11]. The invention of the internet and the emails communications in the last few years revolutionize all industries, markets, banks, services, and educations however health systems stayed behind other sectors to use electronic communication. Emails can reach the most remote areas and can be accessible at anywhere any time when there is an internet. However, health professionals and doctors are among the last to use email communications with their patients [12]. The traditional way which is still implicated in many countries by using letters, face to face consultations and phone calls for communication between patients and their doctors and between General Practitioners and secondary and tertiary centres is time and cost consuming. It cost the countries millions of pounds for paper and letter only. Electronic communication occurs instantly and may reduce unnecessary visit to the doctors and on the same time quick and efficient in raising concerns about serious issues such as medication dosages and correcting important information related to patients’ daily care. The electronic communication with parents or patients is not a replacement for the traditional consultations but it augments the continuity of care to the patients in their homes or holidays and may reduce the need for many consultations.
Electronic communication with patients expand the health care delivery beyond the boundaries of clinic walls. In the last 50 years about 15% of the ambulatory care was delivered by phone calls [12]. Emails offer mutual benefits in the patients-centered-care like it provide immediate accessibility for patients, their concerns addressed quickly, reduce lost time from work and create loyalty of patients to their healthcare providers on the same time reduce the inappropriate internet information surfing by the patients. For many healthcare professionals and doctors the main concern of not using the email or other electronic systems is the breach of patient privacy. However, privacy is a problem with any communications including calls, paper communications and files. Such fear is overblown by using secure hospital electronic system. In fact, most patients understand the privacy risk and willing to bear. In our experience from this study all parents were happy to us their email which is kept secure in the HIS (Hospital Electronic System). On the other hand, when they email us we ask them in our first reply if it is acceptable for them to use the email for our replies and we had no objections from them. We do not use mobile phones, personal computers or out of hours reply unless it is from the hospital internet system.
The question that the electronic communication overburden staff with at work is not true. It has been found from this study that emails take much less time than calls, reach immediate to the patients and less costs than letters and phone calls. It has been shown that telephone call takes at least 10 minutes and may need several calls to get into the line of the patients and a traditional visit takes often more than 20 minutes however doing an email about the same issue takes only 1 to 2 minutes. Despite of that less than 10% of doctors using the email communications [13]. By implementing the email communication with our patients, we managed to reduce the phone calls into almost zero.
Using the electronic emails to communicate with patients is not only adding something new on the traditional practice but it should serve as a way to re-engineer the practice by enhancing the communication and make efficient use of time. In this study during the last two years 2017 and 2018 and based on midterm review of the results the communication work with parents reorganised to allow more and effective use of nurse communication as noted in figures 3 and 5. This will make efficient use of time of both doctor and nurse in the same practice while achieving patients’ satisfaction and reducing complaints.
It has been shown in this study that the reasons for parents’ electronic email communications with the health professional (paediatrician) are comprehensive across all the common and sometime rare illnesses of the children and new-born babies. The commonest illnesses that parents required an answer for via email communications are fever, respiratory symptoms, skin rashes, gastrointestinal issues, appointment, vaccinations and feeding (figure 3). In fact, the miscellaneous queries included wide range of symptoms and illnesses (Table 3). This type of classification enables us to produce written information about some of these concerns and allow us to widen our face to face consultations to cover these subjects such as fever management, red flag signs of different illnesses and the other common concerns mentioned. Likewise, it enables us to gain wider knowledge about these concerns and so as improve our communication skills and ultimately patient’s care. That was one of the factors contributing to reduction of number of emails to the consultant later on.
Some health institutes use guidelines about electronic communication though most of them are about specific clinical speciality such epilepsy, AIDS, and others [14] while other professionals published guides for parents of how to write effective emails to their paediatricians [15]. We do not have a guideline however we had no problem about the emails except rarely parents send attachment of large image that is not allowed to pass through the system and we ask them to resend again via different ways. There were no problems with autoreply compared to phone calls which so many times resulted in auto answering machine. Few cases only raised concerns about acute illness that need immediate assessment and either we arrange to see patients on the same day or advise parents to take child soon to the Emergency Department. When the doctor on leave we usually apply autoreply in which we offer telephone number and extension if the concern is urgent and date of when parents expect feedback. Rarely the email may be overused or misused by parents such as sending several emails per day about trivial or the same issue and in that case, we arrange an appointment soon to have a talk face to face as this may represent underlying problem that parents may need support about it. In our practice parents, themselves requested an email to communicate with us while others feeling happy when we provide them with both the doctor and nurse email. We verbally encouraged them to email us or ask their permission to email them the results. Sometime refill may be done by email or reports as shown in figure 4. Few reports published about the concept of patients view about the use of email communication with their health providers. However, the number of patients who like to use the email with their doctors is more than the doctors who think they need to use it. In a very large study in the USA 70% of patients are willing to use emails with their doctors [16]. Similar number of patients were reported in the UK [17]. Over 4 years prospective use of email communication we had no single report of risks of confidentiality, increase workload, medicolegal concerns, or any other issues. We use autoreply during leaves and public holidays while we had not received autoreply from patients’ emails in reverse to phone calls where we experienced many answering machine messages with different kinds. Emails form suitable way of copying and attaching it to the HIS system in the patient file and what action was taken. It is advisable that when writing an email to parents you think in the same way when documenting a history from patient. Emails from patients and response to them is a medico legal communication like any other consultation and issues like did the doctor scroll through the whole email, how long takes to reply, what was the doctor doing when the email arrive, and how the doctor prioritize their work maybe raised when patient file need to be assessed for medico legal aspect. Hence it is advised that the doctor should read the parents’ or patients’ emails thoroughly, make the response clear, leave open doors for patient to clarify, use secure system in the centre only, patient to confirm receipt, limitation of response to the patient point, avoid more than one reply and if response not swift let them know. The email response should be concise, clear, easy to read, informative and empathetic. When link need to be provided use appropriate, relevant, peer reviewed and up-to-date sites only. Always take cues from the patient’s email such as level of the knowledge of the sender, status of the concerns, and if needed to advise patient to seek urgent clinical review. Medical jargon should be avoided in response likewise acronyms and abbreviations while making the sentences and paragraphs as short as possible. Counselling skill should be applied on writing email too such as avoid making assumptions by reading carefully, match language, acknowledge level of concern, reinforce right steps taken by patients, and ensure phrasing as sensitive as possible.
Electronic email communication with parents provides new way of communication that if used properly it will augment traditional ways of consultations. It is more convenient than phone calls and time and cost saving. It provides flexibility, written information, trail, wide accessibility, and build trust with parents or patients. Emails are storable and can be used to assess different topics and concerns raised by patients for future analysis by audit or study to improve communication with patients and parents.
Unlimited acknowledgments to parents who shared their children concerns by email communications with us that allow us this great opportunity to share the results of this unique study with clinicians and health professionals around the worlds so as they may utilize the same way of sequential communication for a better health care for all children anywhere around the globe.
The authors declare that there is no conflict of interest regarding the publication of this paper.
The data are anonymous and untraceable back to patients. No names or pictures or similar ways of identifications were used.
Copyright: © 2019 Sam Hassan and Rowell Sinlao. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.