Sai Charan1, Venkatesh M Annigeri2*, Akshay Kalavant B3 and Anil B Halgeri2
1
House Surgeon, Department of Pediatric Surgery, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, Karnataka, India
2
Professors, Department of Pediatric Surgery, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, Karnataka, India
3
Assistant Professor, Department of Pediatric Surgery, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, Karnataka, India
*Corresponding Author: Venkatesh M Annigeri, Professor and Head, Department of Pediatric Surgery, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, Karnataka, India.
Received: December 17, 2018; Published: January 22, 2019
Citation: Venkatesh M Annigeri., et al. “Gallbladder Hydrops Secondary to Cystic Duct Stone in Child: A Case Report”. Acta Scientific Paediatrics 2.2 (2019):15-17.
Gallbladder hydrops is very rare in children. It is caused by blockage in cystic duct, which can be either mechanical or functional. The term gall bladder Hydrops refers to a non-inflammatory over distended gall bladder filled with mucus. This entity commonly seen in adults. Here in we report 4 year girl she admitted with abdominal pain with mass then diagnosed as gallbladder hydrops and managed successfully by surgery.
Keywords: Gallbladder Hydrops; Ultrasound; Cholecystitis; Cholecystectomy
Gallbladder hydrops (GBH) or Mucocele of gall bladder is a rare entity in pediatric age group [1,2]. It is caused by blockage in cystic duct, which can be either mechanical or functional. GBH is a term denoting an over distended gallbladder “filled with mucoid or clear and watery content” [3]. HGB is a also rare cause of right upper quadrant mass in children [4-6]. The diagnosis is made when gallbladder content is clear mucous like fluid replacing the green or brown bile. Here in we report 4 year girl who admitted with acute abdominal pain and mass then diagnosed to have gallbladder hydrops and managed successfully by surgery.
A 4 year girl admitted to our emergency department with complaints of pain in the upper abdominal region since 4 days, vomiting since 1 day. There is no history of bowel and bladder movement disturbances, fever and jaundice.
On examination abdomen was flat with tenderness and mass present over the right hypochondriac region measuring about 4 x 3 cm (Figure 1A). Routine blood investigations showed total leucocytes counts 16,500 cells/mm3. Total bilirubin was 0.6 mg/dl with direct fraction of 0.2 mg/dl, rest of all hematological investigations were within normal limits. Ultrasound (USG) abdomen revealed minimal gallbladder wall thickening and 8mm stone located in cystic duct. Plain Computer Tomography of abdomen showed a radio dense calculus in the gallbladder neck region measuring about 8 mm in size (possibly representing the impacted gallbladder neck stone) and gallbladder is distended (Figure 1B).
Diagnostic laparoscopy was planned in view of pain abdomen and mass, on laparoscopy gallbladder was distended and the wall was thinned out. Adhesion were presents in calots triangle and in around the gall bladder. then converted to open by subcostal incision. Through needle aspiration about 35 ml of viscid colorless mucus was evacuated from gall bladder (Figure 2A). After adhesiolysis the extra-hepatic biliary ducts exposed. 8 x 6 mm black colour stone impacted at cystic duct (Figure 1C). Cholecystectomy was performed (Figure 2B). She had uneventful post-operative course and child was discharged after five days. The gallbladder specimen (Figure 2B) was sent for histo-pathological examination which revealed chronic inflammation. In follow up she is doing well and free from symptoms.
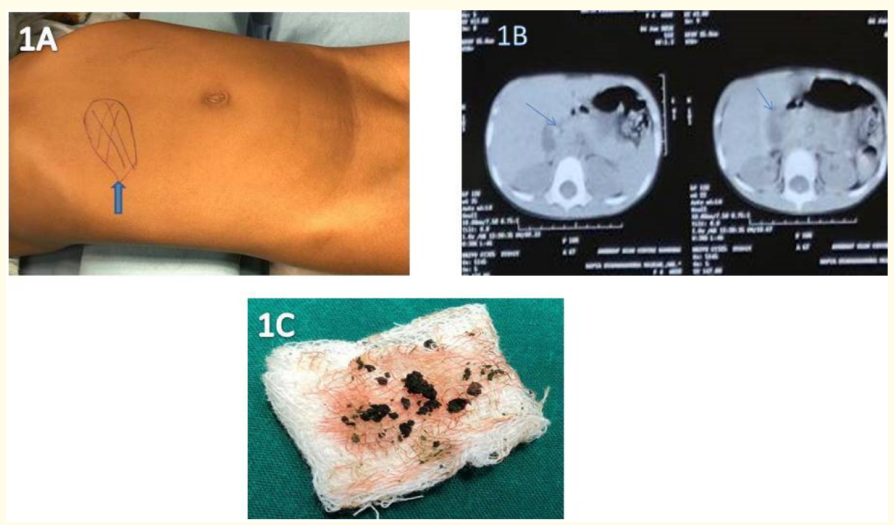
Figure 1: A: Demonstration of site of tenderness and mass( Right Hypochondriac region). B: CT Abdomen showing distended gall bladder and a radio-dense calculus in the neck of gallbladder. C: The calculus removed in pieces from the cholecystectomy specimen.

Figure 2: A: Intraoperative photo showing colourless mucous fluid aspirated from the distended Gall Bladder. B: Cholecystectomy specimen.
Gallbladder (GB) diseases is a very rare entity in pediatric age group [4]. The term gall bladder Mucocele or Hydrops refers to a non-inflammatory over distended gall bladder filled with mucus [1,4-6]. In adults it is more commonly seen when there is mechanical obstruction to cystic duct or gall bladder neck usually by a gall stone [4]. It is a rare entity in children. It has predilection for boys [1,2]. As seen in adults, obstruction of gall bladder outlet by stone is one of the causes of hydrops as seen in our patient. The other causes include mechanical obstruction caused due to neoplasms like gall bladder polyps, congenital strictures, gall bladder parasites like, Clonorchis sinensis, Opisthorchis viverrini, Fasciola and sometimes due to external compression caused by enlarged perihepatic lymph nodes, and liver tumors [1,2]. However, in infants and children Acute Acalculous non-inflammatory Hydrops is associated with Kawasaki disease, Nephrotic syndrome Polyarteritis nodosa, Leptospirosis, Scarlet fever, Staphylococcal infection, Familial Mediterranean fever, and leukaemia [1,2,5,7]. Other causes which increase the risk of Cholecystitis such as exponential weight reduction, prolonged total parenteral, gastric surgeries with disruption of Vagus nerve, hyperlipidemia, hypercalcemia and even biliary conditions such as Carole disease are also mentioned. Hepatotrophic viruses are also mentioned as a cause for Hydrops [2].
Bile is stored and concentrated in the gall bladder. It can store about 1500 ml of bile and can distend if there is an obstruction [4]. In case of a complete obstruction or non-emptying of gall bladder, the bile salts will get reabsorbed by the gall bladder mucosa over time and be replaced by clear, watery mucus [7]. Pathological examination reveals many Rokitansky-Aschoff sinuses which are herniation of mucosa caused due to increased pressures [8]. Prolonged cases can even lead to perforation.
The child presents with varying symptoms and signs but certain features seem to be relatively constant. Pain abdomen in right hypochondria is most common presentation. This pain is present for years until diagnosis. The child frequently has a fever, vomiting and nausea. Often, a specific dietary event such as consumption of high fat foods leads to an acute attack. It can be differentiated from other similar conditions such as acute cholecystitis if the pain persists for more than 6 hours, along with common bile duct obstruction and jaundice. On examination a large palpable minimally tender mass is found in the right hypochondriac region [1].
The workup for gallbladder mucocele should be similar to the ones done for acute cholecystitis. Liver function tests are usually within normal limits, raised bilirubin levels may indicate common bile duct obstruction. An accurate and specific diagnosis of Mucocele of gall bladder can be made from Ultrasonography [1], which shows grossly distended gall bladder of size greater than 5 cm antero-posteriorly with a stone impaction in the infundibulum as seen in our patient and clear fluid indicate possible GBH [3]. Computed tomography is done in case the diagnosis if unclear (in our case patient was referred with ultrasound and computed tomography report) [9]. Literature also mentions the use of Hepato-Iminodiacetic acid scintigraphy in uncertain patients [2]. Cholecystokinin studies improve the quality of tests and they are more specific [3]. The treatment of choice for HGB secondary to cystic duct obstruction is Cholecystectomy either by laparoscopy or open method [4,10]. Intra-operative aspiration of large gall bladder helps facilitate grasping the gall bladder and dissection (as we did in our case). If the patient is acutely ill and considered a poor surgical candidate, open or ultrasound guided cholecystostomy can be done in very sick patients followed by completion cholecystectomy once is the patient is clinically stable [4]. Gallbladder drainage with Endoscopic ultrasound (EUS) guided endoluminal approach have also been described. Acute Acalculous non-inflammatory Hydrops is self-limiting and resolves on its own [6,8,10,11].
Gallbladder hydrops is very rare in children. It should be considered as a differential diagnosis of pain abdomen with right hypochondriac mass in children. Early diagnosis and proper management will prevent complication.
There is no funding and conflicts of interest involved in this study.
Copyright: © 2019 Venkatesh M Annigeri., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.