Karam Husni Abu Shakra1* and Niveen Ahmed Al Foqaha2
1
Senior Specialist Paedodontist, Royal Medical Services, Jordan
2
High Diploma, Specialist Diabetes Educator, Royal Medical Services, Jordan
*Corresponding Author: Karam Husni Abu Shakra, Senior Specialist Paedodontist, Royal Medical Services, Jordan.
Received: November 09, 2018; Published: December 28, 2018
Citation: Karam Husni Abu Shakra and Niveen Ahmed Al Foqaha. “Oral Health in a Group of Jordanian Diabetic Children”. Acta Scientific Paediatrics 2.1 (2019):16-20.
Objective: to evaluate dental and gingival health in a group of Jordanian patients with diabetes mellitus type 1 compared to non- diabetic control group.
Methods: The study sample comprised 120 children of both sexes aged between 4-15 years old. 60 subjects were the test diabetic group and 60 subjects were the healthy control group. The metabolic control of diabetes was categorized into controlled and uncontrolled diabetes subgroups based on glycosylated haemoglobin HbA1c. The gingival status was assessed for all subjects with the gingival index (Löe-Silness). Dental examination included DMFT/dmft index (decayed, missed, and filled teeth) for permanent and deciduous dentition. Non parametric Mann-Whitney U test was used in the statistical analyses
Results: higher mean value of DMFT score was found in the diabetic group, whereas higher mean rank of dmft was noticed in the control group. However, this was not statistically significant. Yet again, no significant difference was observed between the subgroups of the diabetic sample or between both sexes. The moderate gingival inflammation with bleeding on probing was more prevalent in diabetic subjects and represented 71%. Normal gingival appearance with no inflammation and gingiva with mild inflammation were found more common in the control group with a percentage of 54% and 56% respectively.
Conclusion: Despite the fact that no statistically significant differences was observed in the mean DMFT/ dmft index between diabetic and control group, still type 1 diabetes mellitus could play an important role in the dentition and oral health. Children with type I diabetes mellitus could also be more prone to the development of gingival inflammation.
Keywords: Diabetes Mellitus; DMFT/Dmft Index; Gingival Index
Dental caries is an infectious, multifactorial and diet related disease [1]. Plaque bacteria ferment the available carbohydrates from the ingested food and produce organic acids, which causes demineralization of dental hard tissue [2]. Plaque, which usually reflects the oral health, also play a major role in the development of periodontal disease which is related to the gingival health [3]. Oral hygiene, gingival health and dental caries have improved lately in Jordan but, nevertheless prevalence remains high compared to results from developed countries [4].
Diabetes, on the other hand is a metabolic disease characterised by high blood sugar, which results from insulin deficiency [5]. The prevalence of diabetes in Jordan is high and increasing. A recent study in Jordan, found that the age-standardized prevalence of diabetes mellitus was 17.1% and impaired fasting glucose tolerance was 7.8% [6]. Diabetes mellitus type1 accounts for 5% to 10% of cases of diabetes in the United States, Canada, and Europe [7].
The relationship between dental caries, gingival inflammation and diabetes mellitus is complex and depends on many factors such as the type, duration and control of diabetes, the salivary flow and oral hygiene [5]. Despite the fact that diabetes is a very common metabolic disease, and dental caries and gingival diseases are very common oral problems, however, this association has not received enough attention in Jordan. There are no studies in Jordan conducted to evaluate the relationship between these diseases.
The aim of our study was to investigate the occurrence of dental caries and gingival inflammation in a sample of Jordanian children with type I diabetes mellitus and compare it with non-diabetic healthy controls.
The study sample consisted of 120 children (60 children as test group and 60 children as control group), aged between 4-15 year old children. Ethical approval was obtained from the human research ethics committee of the directorate of Jordanian Royal Medical Services.
The test group included 22 boys and 38 girls (mean age10.6 years; SD = 3.7) with Type I diabetes mellitus. Assessment of their metabolic control of diabetes was based on the glycosylated haemoglobin HbA1c. Patients were evaluated at the Department of the Childhood Endocrinology at Queen Rania Hospital for Children in Jordan before sending them to the Paediatric Dentistry Department. The metabolic control of diabetes mellitus was categorized into two subgroups; controlled and uncontrolled diabetes. HbA1c was considered controlled according to American Diabetes Association (ADA) recommendations 2005, when its level was 7.5% to 8.5% in children aged younger than 6 years, less than 8% in children aged 6 to 13 years and less than 7.5% in patients aged 13 to 18 years [8].
The control group, on the other hand, was comprised of 25 boys and 35 girls with a (mean age of 8.8 years, S.D = 3). Children were non-diabetic, healthy and without any reported systemic disease or medications.
Assessment of the dental health status for the test and control group was done in the dental clinic by one dentist. Examination proceeded in an orderly manner from one tooth to the adjacent using a sterile examination set under dental chair light.
DMFT and dmft scores (decayed, missed and filled teeth) were calculated for permanent and deciduous teeth. For mixed dentition each child was given a separate score, one for permanent teeth and another or primary teeth. A tooth considered present in the mouth when any part of it was visible. Caries was diagnosed using WHO recommendations (1997) [9] for oral health surveys.
Therefore, decayed tooth (D,d) was recorded when a carious cavity was apparent on visual inspection or had undermined enamel in a pit or fissure, or on a smooth tooth surface. A tooth with a temporary filling, or one which was permanently sealed but had recurrent caries was also included in this category. Tooth was considered filled (F,f), when it had one or more permanent restorations and without caries anywhere on the crown. Missing tooth (M,m) was recorded whenever a tooth had been extracted because of caries and not as a result of normal exfoliation or trauma.
Gingival health was examined for the main symptoms inflammation. The gingival index according to Löe and Silness (1963) [10] was recorded for the mesial, distal, buccal, and lingual surfaces with a manual periodontal probe. The scores were as follows:
The data were analyzed using an SPSS (version 16.0). The results were expressed by mean values and standard deviations (SD). The differences in the DMFT and dmft scores between the diabetic and non-diabetic sample, between the two subgroups of the diabetic sample, and between genders were assessed by using nonparametric Mann-Whitney U test.
Diabetic group comprised of 60 children, 22 males and 38 females with a mean age of 10.6 years ± 3.7 SD. The number of subjects who were in their primary dentition stage was 9 children, in their mixed dentition 19 subjects. The remainder 32 children were in their permanent dentition stage. The mean DMFT was 2.6 ± 3.3 SD, whereas the mean dmft was 2.5 ± 3.0 SD. Patients who had controlled HbA1c were 31 while patients with uncontrolled HbA1c were 29.
Control group comprised of 60 children, 25 males and 35 females. Mean age was 8.8 years ± 3.0 SD. 11 children were in their primary dentition stage, while 12 children were in their mixed dentition stage. As for subjects in the permanent dentition stage, they were 38. The mean DMFT was 1.2 ± 1.8 SD whereas mean dmft was 3.6 ± 3.4 SD.
However, there were no statistically significant differences in the mean values of DMFT scores between the diabetics and nondiabetics control, although higher mean rank was seen for the diabetic group (p = 0.07). As for dmft scores, higher mean rank was noticed in the non- diabetic control sample but again this was not statistically significant (p = 0.15). The mean DMFT and dmft index for both groups are demonstrated in figure 1.
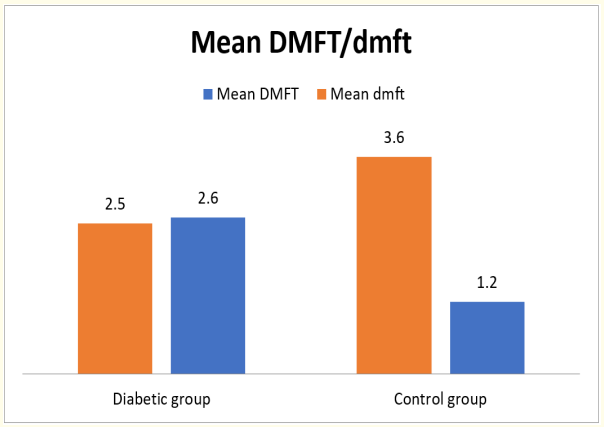
Figure 1: Mean DMFT/dmft in diabetic and control groups.
Furthermore, the mean values of DMFT scores between the two subgroups of the diabetic subjects showed no statistically significant differences (p = 0.73). This was also observed for dmft scores where no significance was found (p = 0.79), though the uncontrolled diabetic patients had higher mean rank. The mean DMFT for the controlled diabetic subgroup was 2.7 (SD = 3.4) and the mean dmft was 2.2 (SD = 2.4). For the uncontrolled diabetic subgroup mean DMFT and dmft were 2.5 (SD = 3.4) and 3 (SD = 3.6) respectively. This is displayed in figure 2.
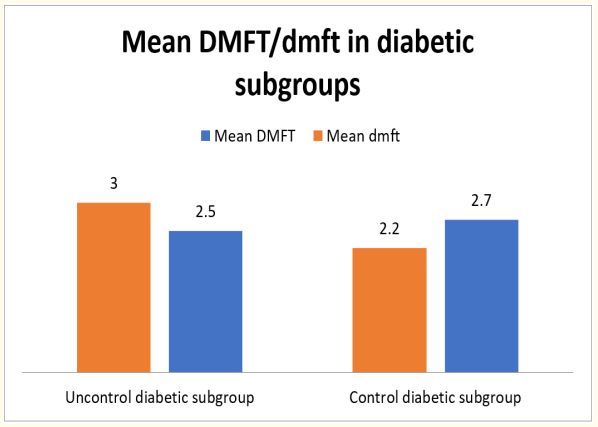
Figure 2: Mean DMFT/dmft in controlled and uncontrolled diabetic subgroup.
Finally, no statistical significance in the DMFT and dmft index was obvious between males and females in the diabetic and control groups (p> 0.05). Means of DMFT and dmft scores in both sexes and in both groups are shown in figure 3 and figure 4.
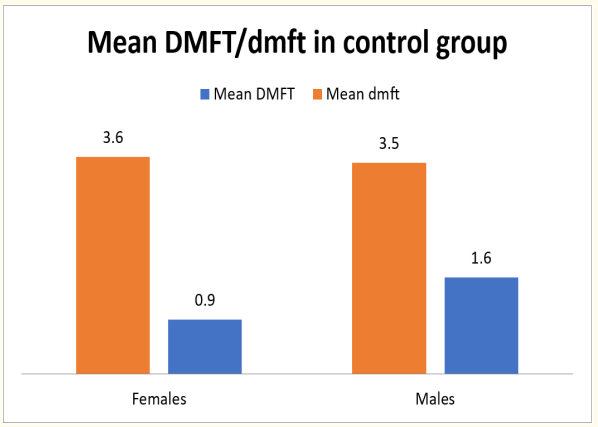
Figure 3: Mean DMFT/dmft between males and females in the control group.
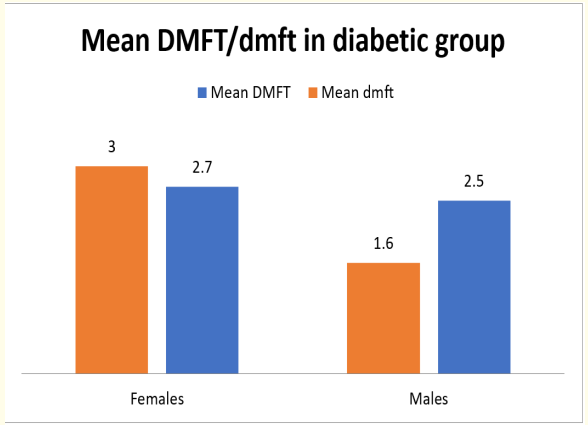
Figure 4: Mean DMFT/ dmft between males and females in the diabetic group.
Regarding gingival health, normal gingival appearance with no inflammation and gingiva with mild inflammation were found more common in the control group with a percentage of 54% and 56% respectively. The moderate inflammation with bleeding on pressure was more prevalent in diabetic subjects and this represented 71% whereas in the control group it was 29%. As for severe inflammation, prevalence was equal between test and control sample. This is shown in figure 5.
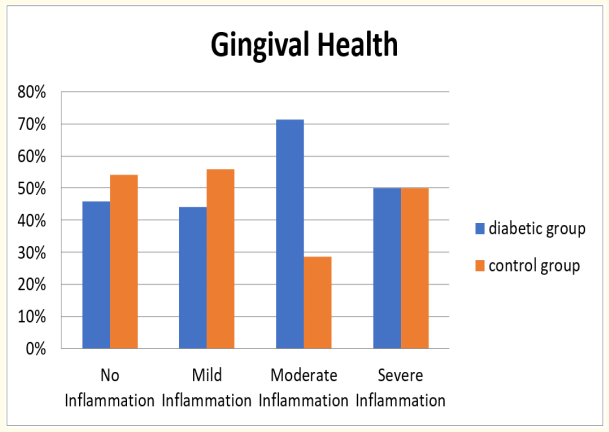
Figure 5: Gingival Health status in diabetic and control group.
The results of studies on the relationship between dental caries and diabetes mellitus type 1 have been variable and no specific association has been identified.11 Some studies have shown that diabetics had lower caries prevalence, despite the fact that diabetic patients have disturbed glucose metabolism, with increased concentration of glucose in blood and saliva combined with alterations within plaque bacteria and decreased saliva flow rate. 12 That was attributed to the sucrose-restricted diet. Furthermore, because of modern management of diabetes, diabetic patient has less restricted diet. This might reduce the significance of the dietary factors as the marker for differences in caries between diabetic and nondiabetic subjects [12].
In Jordan, data regarding prevalence of type 1 diabetes mellitus are very scarce. Furthermore, prevalence of dental caries or gingival disease in diabetic patients is not available in Jordan. However, some studies were conducted regarding the experience of dental caries in healthy children in Jordan. Rajab and hamdan (2002) found the mean dmft scores for children aged 1, 2, 3, 4 and 5 years were 0.2, 1.2, 1.7, 2.1 respectively [13]. Sayegh., et al. (2002) reported that the dmft values found in their study were 3.1 and 4.1 in 4 and 5 year olds respectively. For permanent dentition DMFT index was found to be 2.5 in 12-13 years old was [15]. In our study the mean DMFT for healthy non diabetic children was 1.2, and the mean dmft was 3.6.
As for the mean DMFT in diabetic patient in our study, it was higher than the mean score of the non-diabetic controls, whereas the mean dmft was lower. Orbak., et al. (2008) demonstrated that children with Type 1 Diabetes Mellitus have less caries than non-diabetic children in all the age groups [14]. Bharateesh., et al. (2012) also found the prevalence of dental caries was more in non-diabetics (32.3%) than in diabetics (13.6%) but in adult group [17]. On the contrary, Miko., et al. (2010) reported that adolescents with type 1 diabetes mellitus had a higher mean DMFT score [18]. Whereas, Lalla., et al. (2006) stated that there were no differences in their study between case and control subjects with respect to dental caries [19]. In Sudan, the prevalence of dental caries and DMFT index were higher in the control group than in the diabetic children [20].
Regarding gingival disease in healthy non diabetic children, Sayegh., et al. (2002) reported a prevalence of 66% gingivitis among 4-5 year old Jordanian children [21]. The results of the study that carried out by Nassrawin and Abu Shakra (2010) revealed that the occurrence of gingivitis in a Jordanian sample was 49.1% [22]. In addition, Taani., et al. (2003) found that 43% of their study subjects had bleeding on probing [4].
As regards to the relationship between diabetes and periodontal diseases, it has been well recognized in the dental literature [19]. In our study moderate inflammation with bleeding on probing was more prevalent in the diabetic test group (71%). On the other hand, mild inflammation and no inflammation were more expressed in healthy non diabetics seen. Siudikienė., et al. (2005) recorded healthy gingiva in 87% of the non-diabetic children. They also found mild and moderate forms of gingivitis were more expressed in the patients with diabetes [12]. They explained that was due to high glucose level in blood and gingival fluid which might have caused qualitative changes in bacteria that was responsible for the severity of periodontal problems, observed with diabetes [12]. Orbak., et al. (2008) also reported a prevalence of 69.7% of gingival inflammation in the group of 5 - 9 year old, and 83.7% in the group of 10 - 14 year old subjects with type 1 diabetes mellitus [16]. Glickman, the father of modern periodontology, considered diabetes as a predisposing condition for periodontal disease and not the direct cause. Since diabetes might cause metabolic imbalances in the tissues, which lower the resistance of diabetics to infection, thus, influencing the development of periodontal disease. Besides, vascular changes in diabetes mellitus could result in increased gingival bleeding [16].
Bharateesh., et al. (2012) found the prevalence of periodontal diseases was more in diabetics (92.6%) when compared to nondiabetics (83%) [17]. Lalla., et al. (2007) as well, observed greater prevalence of periodontal disease and tissue inflammation in children with diabetes mellitus.
Children with type I diabetes mellitus could be more prone to the development of gingival inflammation. Although, no statistically significant differences were observed in the mean DMFT/dmft index between diabetic and control group, but nevertheless, type 1 diabetes mellitus could still play an important role in the dentition and oral health. Therefore, patients with diabetes mellitus should learn about the importance of oral health implications of diabetes and should be encouraged to visit the dental clinic regularly.
Copyright: © 2019 Karam Husni Abu Shakra and Niveen Ahmed Al Foqaha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.