K Karavdic1*, S Pandur2, E Milišić1, A Mešić3, A Džananović4 and I Sefić-Pašić4
1
Clinic for Pediatric Surgery, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina
2 Heart Center, Sarajevo, Bosnia and Herzegovina
3
Clinic for Anesthesia and Reanimation, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina
4
Institute for Radiology, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina
*Corresponding Author: K Karavdić, Clinic for Pediatric Surgery, Clinical Center of the University of Sarajevo, Bosnia and Herzegovina.
Received: September 04, 2018; Published: December 26, 2018
Citation: K Karavdić., et al. “A Late-Recognized Left Side Congenital Diaphragmatic Hernia Combined with an Ectopic Kidney in a 9-month-Old Boy Treated by Thoracoscopic Procedure after Previous Successful Treatment of Ventricular Septal Defect”. Acta Scientific Paediatrics 2.1 (2019):12-15.
Renal ectopia is a rare anomaly which may occur due to an abnormal ascent of the kidney. CDH is a rare condition (0.01% - 0.05% of births). Its association with multiple congenital anomalies in various organs is well recognized. Intrathoracic renal ectopia with concomitant congenital diaphragmatic hernia (CDH) is extremely rare. The reported incidence of intrathoracic renal ectopia due to CDH is 0.25%.
The authors report on a a 9-month-old boy with late-presenting left sided congenital diaphragmatic hernia associated with intrathoracic ectopic kidney treated by video-assisted thoracoscopic surgery (VATS) after successful treatment of ventricular septal defect.
Keywords: Renal; Ectopia; Diaphragmatic Hernia Thoracoscopic
Renal ectopia is a rare anomaly which may occur due to an abnormal ascent of the kidney. CDH is a rare condition (0.01% - 0.05% of births). [1]. Its association with multiple congenital anomalies in various organs is well recognized. Intrathoracic renal ectopia with concomitant congenital diaphragmatic hernia (CDH) is extremely rare.The reported incidence of intrathoracic renal ectopia due to CDH is 0.25% [2].
Thoracic ectopia of the kidney may be a congenital anomaly or secondary to herniation through a congenital or acquired diaphragmatic defect; males and the left side are more commonly involved [3].
CDH is a major surgical emergency in newborns as it may be lead to pulmonary hypoplasia, or may be related to persistent fetal circulation, and other coexisting congenital anomalies [4]. The authors report on a a 9-month-old boy with late-presenting left sided congenital diaphragmatic hernia associated with intrathoracic ectopic kidney treated by video-assisted thoracoscopic surgery (VATS) after successful treatment of ventricular septal defect previously operated by pediatric cardiac surgeons.
Patient, 9 months old boy, was admitted to the Children's Clinic for the operation of a ventricular septal defect which was closed with polytetrafluoroethylene (PTFE) patch by pediatric cardiac surgeons. The postoperative cardiovascular course was satisfactory. An elevated left diaphragm is recognized on the preoperative Rtg image completely incidentally, in a routine RTG chest recording as part of preoperative preparation for heart surgery (Figure 1).

Figure 1: Chest X-ray air-filled loops of the bowel in the left hemithorax and a paucity of gas in the abdomen. The left diaphragm is not discernable and there is an mediastinal shift to the right site.
Patient had a satisfactory cardiorespiratory status. Indicates CT: "... left intrathoracally located left kidney, perirenal fat and intestine, thin and and small bowel located in the left chest cavity, in the left lung area the atelektasis zones and the left lower lobus of the lungs. Mediastinum is moved to the right side“ (Figure 2,3).
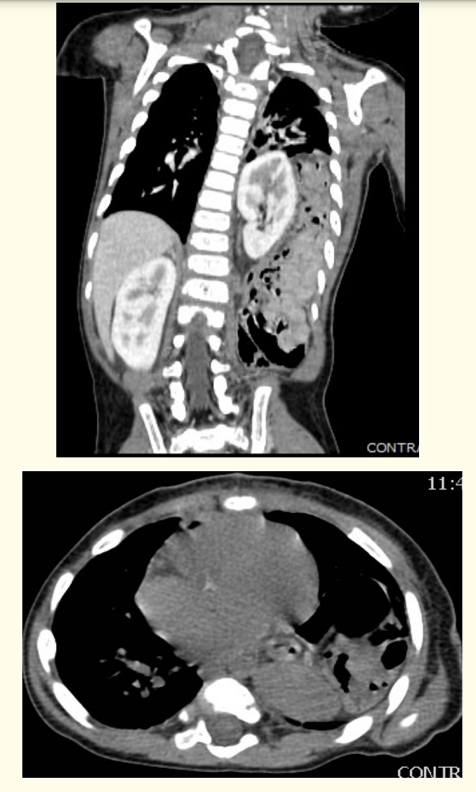
Figure 2 and 3: Thorax CT showing herniation of bowel and kidney into the left side of the thorax.
Echocardiography showed a small, hemodynamically insignificant ENS, no spills, vegetation and signs of thrombosis .. contractility is preserved. FS 37%. Pediatric cardiologist orders Lasix and Aldactone as therapy.
We have indicated surgical treatment of left-sided CDH and kidney ectopia, on the advice of a cardiologist and a cardiac surgeon, we waited 6 weeks after cardiac surgery. A pneumothorax was created using insufflation with low pressure (4 mmHg) and low flow (1.5 l/min). Thoracoscopy revealed a large posterolateral defect of the left diaphragm . A bulge in the kidney and small bowel loops were seen posteriorly (Figure 4,5).
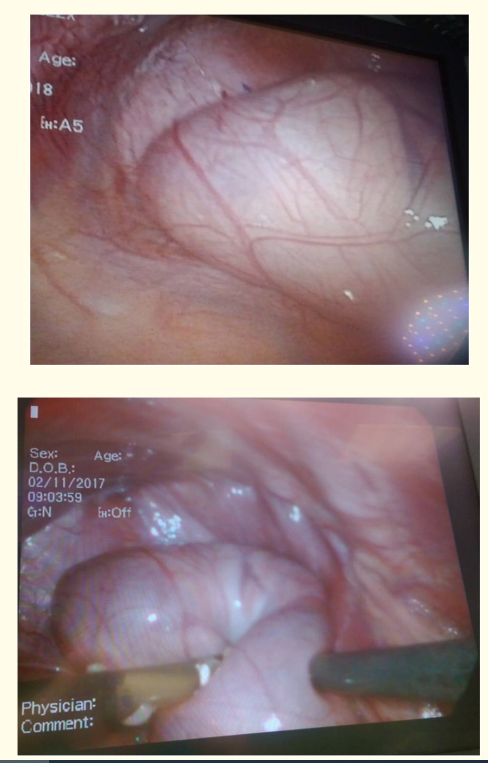
Figure 4 and 5: Thoracoscopic view of the hernia sac showing kidney and small bowel loops impression.
The hernial contents were reduced and plication of the diaphragm was done, taking care to avoid renal and/or vascular injury with 2-0 non-apsorbale suture (Figure 6,7).
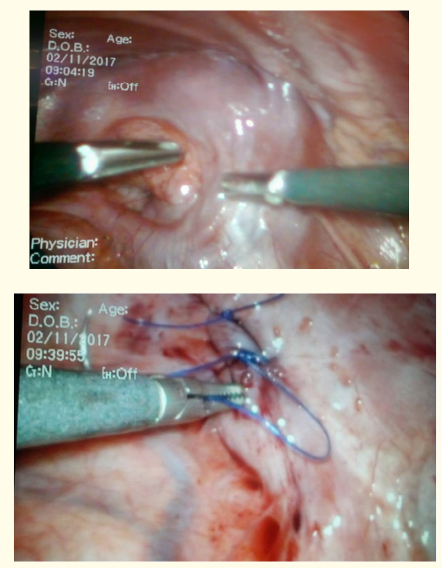
Figure 6 and 7: Defect of the diaphragm after the renal reposition into the abdominal cavity and closure the diaphragm with 2-0 non-resorptive suture.
Postoperative recovery was uneventful. Abdominal ultrasonography showed the kidney was located on the normal position without hydronephrosis. Control chest radiography showed the satisfactory appearance of the left diaphragm and the chest wall had a satisfying cosmetic look (Figure 8,9).

Figure 8: The appearance of the chest at the tenth postoperative day.

Figure 9: The control Rtg chest shows the normal appearance of the left diaphragm.
Bochdalek congenital diaphragmatic hernia arising due to failed closure of the pleuroperitoneal ducts during the 4th and 12th weeks of gestation [5]. It was first described by Vincent Alexander Bochdalek, a Czech anatomist in 1848.
The left sided hernias are five times more frequent than the right, because of earlier closure of the right pleuroperitoneal canal than the left. The ectopic kidney is usually pelvic, iliac, abdominal, thoracic, contra lateral, or crossed [6]. Incidence of intrathoracic kidney is 1 in 16,000 populations while CDH has a reported incidence of 1 in 2500 - 4000 live births [7].
Ectopic kidney is slightly common on the left side, as in our case [8,9]. The intrathoracic location of an ectopic kidney is the rarest with a reported incidence of 5% of all ectopic kidneys. The association of a Bochdalek hernia and intrathoracic renal ectopia is at 0.25%. Thoracic kidneys are classified into 4 groups: thoracic renal ectopia with closed diaphragm, eventration of the diaphragm, congenital diaphragmatic hernia, and traumatic rupture of the diaphragm with renal ectopia [10]. The ectopic kidney has been known to be associated with many other defects, but we did not find a report in the literature that it was associated with ventricular septal defect.
In majority, the thoracic kidney is benign and asymptomatic and detected incidentally on chest imaging as in our case when we found it as an incidental finding during preoperative treatment of cardiac surgery [11]. Chest radiographs are not appropriate, CT scan would be better for diagnosing diaphragm defects.
Thoracoscopic repair was possible. Creation of a pneumothorax using insufflation with low pressure (4 mmHg) and low flow (1.5 l/ min) is enough to reduce hernial contents [12]. The closure of the defect is with non-apsorble suture. Regular Rtg control and Echo controls are required for a period of 6 months. It is necessary to monitor the condition of the diaphragm and the condition of the kidneys [13]. A greater number of cases would be necessary in order to gain experience and bring the correct guidlines.
The association of ventricular septal defect ,diaphragmatic hernia and renal ectopia is rare.
Thoracoscopic repair of the diaphragmatic defect was feasible and beneficial and should be performed in all cases of late presentation of the congenital diafragmatic hernia.
Copyright: © 2019 K Karavdić., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.