Ana Maria Davițoiu1, Ana Mihaela Mitu2, Alexandra Andrada Bojescu3, Elena Truță4*, Mihai Ionică5,6
1Clinical Emergency Children Hospital “Victor Gomoiu”, Bucharest, Romania
2“Ana Mihaela Mitu” Psychology Cabinet, Bucharest, Romania
3University for Medicine and Pharmacy “Carol Davila”, Bucharest, Romania
4University “Titu Maiorescu”, Bucharest, Romania
5Military-Medical Research Center, Bucharest, Romania
6University “Politehnica”, Bucharest, Romania
*Corresponding Author: Elena Truță, University “Titu Maiorescu”, Bucharest, Romania.
Received: October 15, 2018; Published: November 23, 2018
Citation: Elena Truta., et al. “A Study Regarding the Interrelation between a Good State of Mind as an Indicator of Life’s Quality and Psychotherapy at Children with Attention Deficit Hyperactivity Disorder”. Acta Scientific Paediatrics 1.5 (2018):15-20.
Objective: The estabilishment of a link between a good state of mind as an indicator of the quality of life and the intervention of the psychoterapy at children with ADHD.
Summary: During one year, 50 children from the rezidential institution for children “SOS Children's Villages” Bucharest, where included in our research. The children were distributed in two groups: Group A which consisted of 25 children (12 girls, 13 boys) who were not diagnosed with ADHD and Group B which consisted of 25 children (14 boys, 11 girls) who were diagnosed with ADHD. Initially, the two groups were subjected at a psychodiagnostic battery of tests, one of them being the “Evaluating the Quality of Life of children with ADHD questionaire” elaborated by us, particularly for this research, with the purpose of highlighting the direct link between the children quality of life and their ADHD symptoms. Subsenquently, the children from group B benefited of a psycotherapy protocol which combined the strategies of the short therm psychodynamic psychotherapy. The emotional wellbeing average values of the children from group B and group A were significantly different at the beginning of our program, and at the end the difference were higly reduced according with the statistical point of view.
Conclusion: There is a strong connection between emotional wellbeing, as an indicator of quality of life, and psychotherapy at children with ADHD.
Keywords: ADHD; Emotional Wellbeing; Quality of Life Assessment Questionnaire
The Attention Deficit and Hyperactivity Disorder (ADHD) is defined by The American Academy of Pediatrics as being the most common childhood neuro behavioral disorder which can profoundly affect the academic performances, the wellbeing and the social interactions of the child [1].
The studies performed on children that were diagnosed with ADHD marked out that ADHD is one of the most common psychiatric disorder seen in childhood whose symptoms persist during teenage and adulthood in more than 50% of the cases studied [2,3].
The clinical diagnosis is based on medical, psychological, behavioral and educational comprehensives evaluations. The diagnosis criteria are forecasted by DSM – V and ICD – 10 [4,5].
During childhood, ADHD is diagnosed in a ratio of five boys to one girl. This is explained by the fact that during childhood the boy’s behavioral manifestations resemble to hyperactivity and violence, whereas the girls behavioral manifestations resemble to chronic tiredness and attention problems; those symptoms can be easily ignored and therefore girls are less diagnosed and treated for ADHD [6].
The studies performed on families, twins and adopted children marked out that ADHD has a familial component and a hereditary component, the hereditary component being the main risk factor [7]. The risk of being diagnosed with ADHD is 4 to 10 times bigger for close relatives. Studies performed on twins that were diagnosed with ADHD during childhood and teen years have highlighted the inheritable component of the diseases in 76% of the studied cases [8].
The same studies reveal that the genetics are the base of the persistence of the behavioral manifestations during adulthood [9].
It is believed that the molecular genetic studies will elucidate the mechanism by which ADHD diagnosed in childhood persist or remit in during adulthood. In this way could develop new ways to extend disease prevention in adulthood. In this sense one of the assumptions is issued by J. Halperin which suppose that there is a connection between ADHD and premature cortical dysfunctions, while remission of symptoms is closely related to the maturation of executive control. Cortical and subcortical balance functions induce remission or persistent ADHD symptoms [10,11]. Discovered genetic variations in dopamine D4 (DR4) and D5 (DR5), in dopamine transporter (DAT1), in dopamine beta hydroxylase genes (DB4), in 5-hydroxytryptamine receptor 1B (HTR1B) and the serotonin transporter (5HTT), synaptosomal associated protein (SNAP 25), explain 3.2% of ADHD variation symptoms [8,12]. Recently were identified and other changes in genes like Cadherin – 12 genes (CDH 12).
Quality of life is a complex concept with many sides, is this state of good physical, material, social, emotional, of personal development and activity. It is used as a measure of discretion in several areas: medicine, economics, philosophy, etc. It refers to the more or less quality of human life but has no universally accepted definition by specialists.
Quality of life is the term most multidisciplinary found in current use, poorly used, so should be removed from the dictionary [13]. It is located phrase on everyone's lips, but nobody knows what to do with it [14].
The differences in the definition of quality of life come from the description and interpretation of psychological processes through the concepts and different ways of communications [15].
The position the individual or group in society, social and political factors affect the meaning of the concept of quality of life. The strength of the concept is just his multidisciplinary, but as his generality is higher the power of analytics drops [16].
In the 60s, in the US, it was thought that the economic development alone positively affects the quality of life. It was found, however, that economic development was not enough to describe the quality of life. Although there was burgeoning economy, they faced a high rate of violence, crime, public disorder and degradation of the environment. While assessing the quality of life the social factors should be taken into account. Therefore, the policy of increasing the quality of life will use methods tuned to correct the existing social and economic relations [17].
When we define quality of life we often ask, who is being evaluated: the individual, the society or some specific groups (children with ADHD, women’s health) [18]?
A second question that arises is: What quality of life we wanted to define? Objective quality of life (individual standard of living) or subjective quality of life (subjective way in which each measure his own life - contentment, happiness, fulfillment)?
According to Allardt a better life is defined as: "to have" (material needs), "to love" (social needs) and "to be" (personal development).
According to Veenhoven there are four basic qualities of life: the ability of individuals to overcome life's problems, adaptive potential, how each individual judges their own life, life satisfaction and subjective well-being.
The literature mentions a link between the quality of life level and manifestation of ADHD symptoms.
The quality of life is a multidimensional concept which includes the comprehension of the individual’s development within communities, as well as the matter of how much are the psychological processes being influenced by environmental factors and the man’s meaning of his personal life, like the result of the global evaluation from the point of view of the human person, of his own life [19].
Quality of life refers to both, the objective conditions under which human life unfolds and the subjective way in which each individual percieives his/her own life - the state of satisfaction, happiness and fulfillment [7].
The study’s interests are the psychological perspective (subjective) regarding the quality of life which refers to the perceptions, estimations and strategies that are applied by the individual to his current situation and to the comparison that results with his personal needs, values and expectations.
Compared to the impact that ADHD has on the quality of life of the individual, summing: education, life style, individual evolution; researches have shown that the majority of children with ADHD struggle with: learning difficulties (45.5% vs. 13% at healthy children), failing or dropping out of school (70.9% vs. 21.3%), sleep disorder, low self-esteem, smoking, drugs use (52% vs. 24%) [20].
In the case of ADHD, there is increasingly more evidence in literature showing that the prognosis and quality of life depend on the patient's mental balance and psychological processes that can modulate or stimulate the upper portion of the brainstem.
Zigmond and his team conducted a review of studies on patients with ADHD who received psychological intervention, assessing symptoms reduction rates. They watched the most commonly used types of psychological interventions: psycho-education, behavioral training, individual psychotherapy and group interventions, highlighting their positive impact on physical and mental health [21].
Emotional wellbeing, as an indicator of life’s quality, comprises: positive emotions, negative emotions, self-esteem and personal beliefs [22]. This indicator is included in our questionnaire, in which we turned towards measuring the harm, self-esteem and personal beliefs.
The negative effects are considering the intensity with which feelings are felt as: guilt, the desire to cry, fear, lack of joy of life. The frustrations or lack of understanding can generate violence or retirement into solitude. This section aims at finding solutions for the prevention of child failure to adapt often fail to seek redress false - alcohol, tobacco, drugs, excess of every kind, violence.
Self-esteem many of our reactions are related to the representation we have about our self. A high self-image is characterized by: low aggressiveness, confidence, optimism, acceptance of differences.
Personal beliefs concern the way in which children have the capacity to appreciate the power of learning, memory, attention, intention, willingness to take a decision, assign values to objects and experiences. All are able to give meaning to existence and to ensure the overall feeling of wellbeing. The source of comfort and security, they rely on a sense of belonging to the intelligible world, enhancing motivation for a harmonious adaptation willingness to act independently confirming thus the personality.
The study was conducted between 2013 – 2014. Children from orphanage "SOS Children's Villages" Bucharest were included. Evaluating and psychotherapeutic treatments were conducted with the children’s and their legal representatives’ consent. The study included 50 children divided in two groups: Group A included 25 children (12 boys and 13 girls) without a diagnosis of ADHD and Lot B consists of 25 children (14 boys and 11 girls) diagnosed with ADHD.
Inclusion criteria: Children aged 7 - 15 years; children with ADHD diagnosed and undiagnosed.
Exclusion criteria: Psychiatric diagnoses associated with (autism, psychosis, mental deficiency), associated neurological disorders (paresis, cerebral palsy).
The statistical analysis was conducted based on the Student test even.
The psychological assessments were made with a " Battery of psychodiagnostic tests" presented below.
The questionnaire presents an objective method for assessing and addressing the group with the age between 7 and 14 years. It was built, analyzed, pre-tested and completed in a study conducted in the " SOS Children's Villages, on a sample of 25 patients diagnosed with ADHD.
The method used for the clinical trial included the following.
Group A includes 25 children (12 boys and 13 girls) who weren’t diagnosed with ADHD and Group B consists of 25 children (14 boys and 11 girls) diagnosed with ADHD.
Group A has been used as a reference to evaluate the quality of life. Children from this group have been asses with the “Quality of Life Assessment Questionnaire”, once at the beginning of the study.
Group B was used as experimental group in evaluating quality of life. The children evaluated have benefited of a “protocol of psychotherapy” which combines short psychodynamic therapy strategies. The therapeutic approach was centered on building personal identity to children. The therapy’s goal was to help children feel confident, to help them see the world around them as it really is. The pursued therapeutic techniques and objectives were adapted to the particularities of each child, given the fact that each child is unique, and we cannot extrapolate the same contingency plan for a child to another just because the two are suffering from the same type of mental disorder.
The protocol covered 14 individual therapy sessions for each child with ADHD included in the study and 8 sessions of group therapy (three groups). We tried to make the foster parents understand the characteristics of children with ADHD and prepare them to help the patients manage and mitigate the difficulties created by these characteristic features, during special sessions. Strategies were developed to increase prosocial behaviors and eliminate the inappropriate remains.
The protocol consisted of 8 sessions of group therapy for each caregiver included in the study. The groups were composed up of 6 - 8 participants. Please note that the meetings with the foster parents started before the children’s therapeutic sessions, and in this way by the time the children began the treatment the caregivers could apply what they have learned.
The 25 children (aged 7 to 15) were diagnosed with ADHD at different ages. They have been divided into two groups (7 - 10 years) and (11 - 15 years). In the age group (7 - 10 years) there were 19 diagnosed children, representing (76%). The causes of a medical evaluation of a rate so high in this age group, could be entry into the school system and the difficulties to adapt to it. Among children diagnosed at this age was registered the highest proportion of those who had ADHD, attention deficit hyperactive form. These data are consistent with the specialty literature. Children’s consultation at this age group was frequently performed at the teacher’s requests who was upset by the impulsivity’s or hyperactivity’s manifestations like: motor restlessness, the continuous tendency to run and jump, the inability to remain seated during working hours and the accidents that happen really often especially during breaks.
In the age group 11 - 15 years there were 6 diagnosed children (24%). For the diagnosis of ADHD, the following were highlighted: poor school performance to cognitive possibilities of the subject, failure or drop out, orientation towards risky behaviors.
The two groups were similar regarding the number of children and their gender. From these points of view, the two subgroups are homogeneous, figure 1.
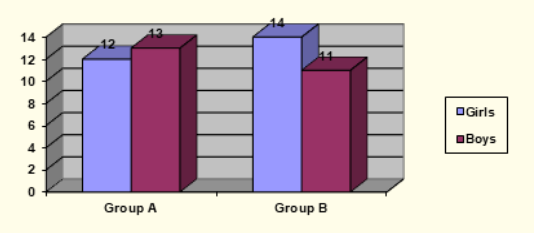
Figure 1: The gender distribution in the subgroups studied.
In the case of SBE variable, assessments carried out prior psychotherapeutic treatment, highlighting the following: A lot’s average was (average) A = 5.72, (Standard Deviation) SD = 2.73 and (Average Standard Deviation) ASD = 0.55 whereas group B’s average was A = 8.32, SD = 3.12 and ASD = 0.55, which indicates that this variable in the two groups has small dispersion values.
In the subgroup AB had A = 4.25, SD = 2.38 and ASD = 0.69 and subgroup AF had A =7.07, SD = 2.36 and ASD = 0.65, which indicated low dispersion values.
The subgroup had BB, A = 8.36, SD = 3.32 and ASD = 0.9 and BF subgroup had A = 8.3, SD = 3 and ASD = 0.91, which indicated a low dispersion values, figure 2.
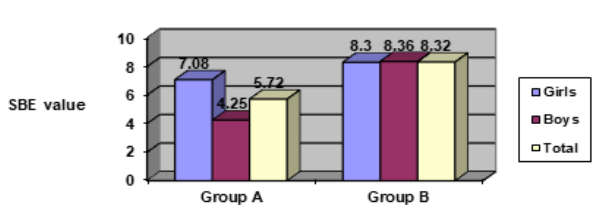
Figure 2: The emotional wellbeing considering groups and sexes.
The odd Student Test shows that the average values differ significantly between groups (p < 0.003), the average value SBE of group A was lower than the average value SBE of group B with 2.6 points. On the frame of differentiated by sex sublots, the average of the emotional wellbeing does not significantly differ relative in the case of group B (p > 0.1), but there is a significantly differences inside of group A (p < 0.007). Variable emotional wellbeing after non-pharmacological treatment showed the following: the average emotional wellbeing (SBE) of group B after treatment was A = 7.12, SD = 2.37 and ASD = 0.47, which shows a normal dispersion value, figure 3.
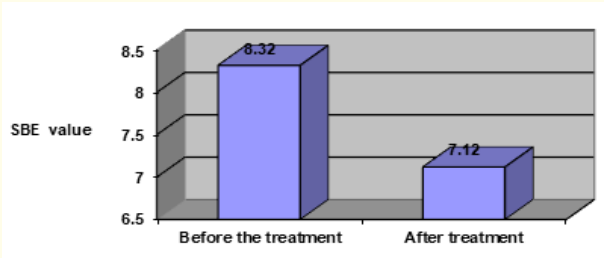
Figure 3: Evolution of emotional wellbeing of group B before and after the treatment.
The Even Student Test shows that the differences average of the emotional wellbeing obtained after non-pharmacological treatment are significantly different to those originally obtained statistically from the zero value (p < 0.003). The emotional wellbeing improved by 1.2 (14.4 %).
In girls case, the average emotional wellbeing of group B after treatment was A = 7.5, SD = 2.34 and ASD = 0.71, which shows a small values dispersion, figure 4.
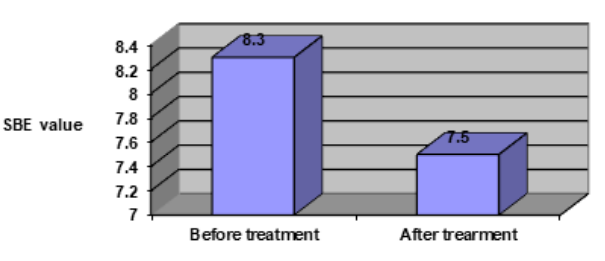
Figure 4: Girls emotional wellbeing improvement in group B.
The Even Student Test shows that the average differences of the emotional wellbeing obtained after non-pharmacological treatment are relative to those originally obtained, don’t differs significantly from the zero value (p > 0.1) although emotional wellbeing was improved with 0.8 points (9.6%).
In the boy’s case, the average after treatment emotional wellbeing of group B was A = 6.86, SD = 2.45 and ASD = 0.65, which shows a small dispersion of the values figure 5.
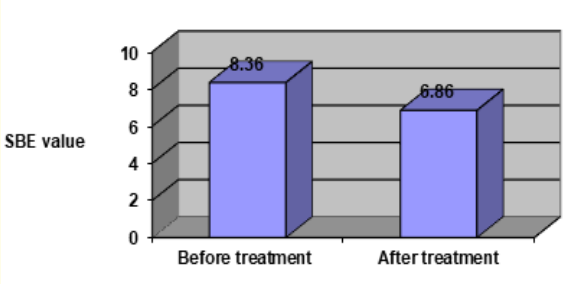
Figure 5: Emotional evolution of boy’s wellbeing in group B.
The Even Student Test shows that the average differences of the emotional wellbeing obtained after non-pharmacological treatment relative to those originally obtained, differs significantly from the zero value (p < 0.01); the after treatment averages were improved with 1.5 (18 %).
From the results, it appears that boys had a significant emotional wellbeing increase compared to girls whose growth is not statistically significant.
There is a direct link between emotional well-being, as an indicator of quality of life and psychotherapy, at children with ADHD.
Copyright: © 2018 Elena Truta., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.