Evaluating the efficacy of surgical fixation in multiple ribs fracture and flail
chest in failed extubation patients: A one year follow up study
Rahul Kakran*1, Vipin Tyagi2, Ashish Agarwal3, Vinay Sharma3, Pankaj Agarwal4, Alok Tripathi5, Saurabh Maheshwari5, Kamaldeep Yadav6, Praveen Kumar7 and AK Singh8
1Senior Consultant Orthopaedic Department, Yashoda Hospital, Ghaziabad UP, India
2H.O.D Orthopaedic Department, Yashoda hospital, Nehru nagar, Ghaziabad, U.P., India
3DNB Orthopaedic,Yashoda Hospital, Nehuru Nagar, Ghaziabad, UP, India
4 H.O.D Radiology Department, Yashoda Hospital, Nehuru Nagar, Ghaziabad, UP, India
5Radiology Department, Yashoda Hospital, Nehuru Nagar, Ghaziabad, UP, India
6Department of Critical Care, Yashoda Hospital, Nehuru Nagar, Ghaziabad, UP, India
7Department of Emergency Medicine, Yashoda Hospital, Nehuru Nagar, Ghaziabad, UP, India
8Department of General Surgery, Yashoda Hospital, Nehuru Nagar, Ghaziabad, UP, India
*Corresponding Author: Rahul Kakran, Senior Consultant Orthopaedic
Department , Yashoda Hospital, Ghaziabad UP, India.
Received: June 18, 2024; Published: August 12, 2024
Abstract
Aim: The aim of this study was to examine the long-term patient outcomes associated with pain, physical function and Quality of life after surgical stabilization of multiple rib fractures or flail chest in failed extubation patients.
Objective:
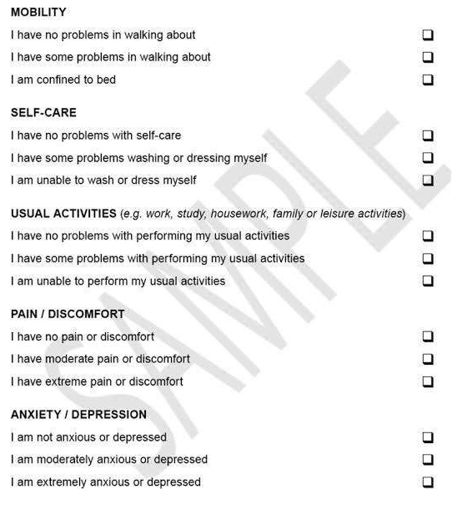
- To assess pain, local discomfort, breathlessness, physical function and analgesics and quality of life according to EQ-5D-3
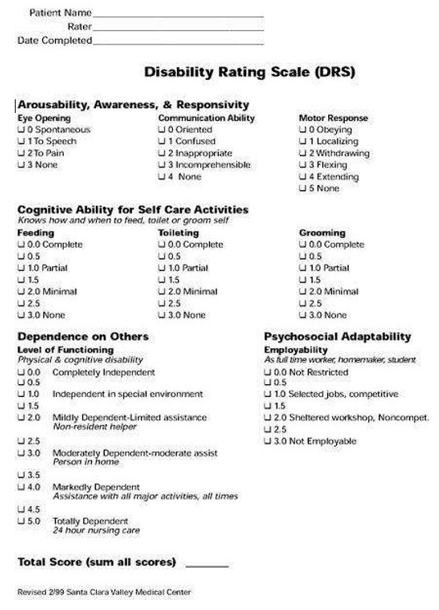
- To assess Physical function of the patient post operative by using the Disability Rating Index (DRI) questionnaire and pain post operative using visual analogue scale (VAS).
Method
- In this Ambispective observational study, we included 10 patients with multiple rib fractures or flail chest as per the
- The patients were selected according to the inclusion and exclusion
- The patients were operated between 2022and 2023 at Yashoda Superspeciality Hospital, Nehru Nagar,
Results
- Of the 10 patients operated three were excluded due to lost to follow
- The proportion of patients seen at follow-up with pain at rest and local discomfort decreased from 7% to 14.2% between 6 weeks and 1 year after surgery with standard deviation of 2.12(30.33%).
- Problems associated with pain on breathing and breathlessness decreased progressively from 71.4% to14.2% at the end of 1 year with standard deviation of 1.63(23.44%)
- Despite enduring pain, there was a significant decrease in the proportion of patients using analgesia from 7% to 14.2% after 1 year with standard deviation of 1.87 (26.75%).
The pain and local discomfort measured by Visual Analogue Scale (VAS) improved significantly over time: mean VAS was 6.14 (5- 8) at 6 weeks, 4.28 (3-5) at 3 months, 1 (0-2) at 6 months and 0.7 (0-2) after 1 year with standard deviation of 2.27.
- Quality of life significantly increased between 6 weeks to 1 year following
- Physical function increased significantly over
- Mean Disability rating index was 2 (14-18) at 6 weeks, 12.57 (11-14) at 3 months, 1.4 (0-3) at 6 months and 0.7 (0-2) at the end of 1 year with standard deviation of 6.8.
Conclusion
- Patients who underwent surgical plate fixation of multiple rib fractures and flail chest (on ventilatory support) showed a gradual improvement in symptoms associated with pain, physical function and Quality of life which continued Throughout the first post- operative
Keywords: Surgical Fixation; Multiple Ribs; Extubation Patients
Introduction
Multiple rib fractures occur in 10% of poly-traumatized patients due to blunt, high-energy trauma [1] and can lead to unstable thoracic cage injuries or flail chest [2] with respiratory insufficiency. Whilst conservative management with analgesics and ventilator support has been the conventional treatment for flail chest, this can entail long hospitalization with immobilization, which leads to complications, such as pulmonary infections and long- term disability with chronic pain [3,4]. Recently, a number of new fixation devices and better techniques have been developed for surgical treatment of rib fractures [5].
Three small, prospective, Randomized Controlled Trials (RCTs) suggest that surgical management of flail chest may decrease the need for ventilator support and intensive care [6-8].
In our clinical setting, we have found plate fixation of rib fractures to be a safe method with a low rate of complications and a reduced time and need for ventilator treatment in comparison to conservatively managed [9].
Our patients were reported to have experienced mild disability, pain at rest, local discomfort after 6 months [10].
Method and Materials
SAMPLE SIZE- 10 patients who underwent surgical fixation of multiple rib fractures as a result of blunt trauma.
The no. Of patients having multiple ribs fractures which are unable to get extubated because of that is quiet a lot but there is lot of debate among the treating physicians, regarding whether to operate these cases or to manage them conservatively. So sample size is a limitation here.
- Type of study: Ambispective observational study.
- Place of study: Study was done at Yashoda hospital and Research centre, Nehru Nagar Ghaziabad, Uttar Pradesh.
- Period of study: From 2022 till 2023
- Investigations: Xray chest-PA view and 3D CT reconstruction.
Pre-operative Three-Dimensional (3D) reconstructions of Computer Tomography (CT) images of the thorax were used for planning the surgical procedure.
Patients were intubated with a double lumen endotracheal tube. A non-muscle sparing thoracotomy was performed to clean out hematoma and debris, identify and, if necessary, manage intra- thoracic injuries.
Fixation System consisting of pre shaped angular locked plates in titanium and S.S wires was used to stabilize rib fractures.
Post-operative pain was managed using either an intrapleural or epidural catheter with adjunct, oral pain medication.
Intravenous broad-spectrum antibiotic therapy was given prophylactically until the chest tubes had been removed.
Low-molecular weight heparin was given subcutaneously as thrombotic prophylaxis.
Patients were assessed at 6 weeks, 3 months, 6 months and 1 year post-operatively using a standardized questionnaire concerning pain, local discomfort, breathlessness, physical function and analgesics and Quality of life according to EQ-5D-3 L [11].
Physical function was estimated by using the Disability Rating Index (DRI) questionnaire [12] and pain was estimated using visual analogue score (VAS).
A chest X-ray was taken at 6 weeks, 3months, 6 months and 1 year post-operatively to assess the presence of lung disease and implant dysfunction or migration.
EQ-5D-3 L Questionnaire
X
![]()
X
![]()
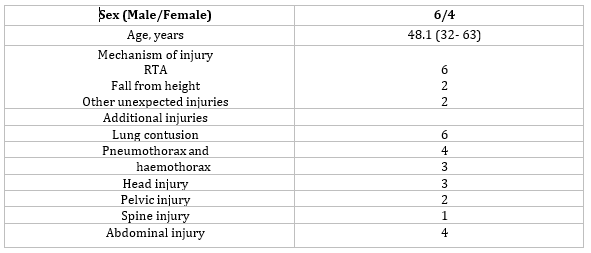
Demographic data
X
![]()
Inclusion criteria
- Flail chest defined as three or more adjacent ribs each fractured in more than one location with respiratory insufficiency
- Failed extubation patients due to flail chest or multiple ipsilateral/ bilateral ribs fracture
- Multiple rib fractures (>4) with respiratory insufficiency and also in need of a thoracotomy due to bleeding or air leakage.
- Patients with severe head injury and spinal cord injury.
- ≥3 rib flail not requiring mechanical ventilation
- ≥3 ribs with severely displaced fractures (bi-cortical displacement)
- ≥3 ribs with mild to moderate displacement and 50% reduction of expected forced vital
- capacity percent despite optimal pain management.
- Symptomatic non-union
- Severe displacement found during a thoracotomy for another reason.
Exclusion criteria
- Contaminated field
- Severe lung contusion requiring prolonged mechanical ventilation
- High cervical spine injury requiring mechanical ventilation.
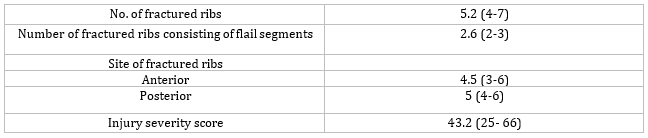
Injury description
X
![]()
Case 1
- Case of 38 years old male
- RTA with Polytrauma with sternum fracture and right clavicle fracture.
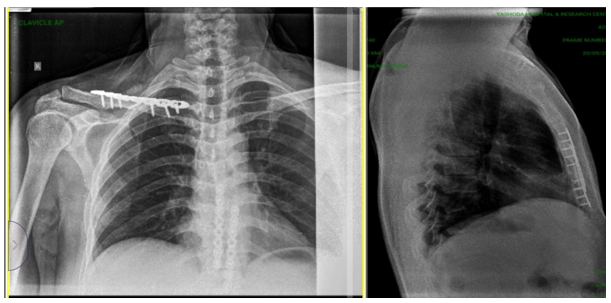
Pre op x-rays showing right clavicle fracture with sternum fracture
X
![]()
Pre op CT scan film showing oblique sternum fracture
X
![]()
Intra op image showing sternum fixation with multiple plates and screws
X
![]()
Immediate post op x-rays
X
![]()
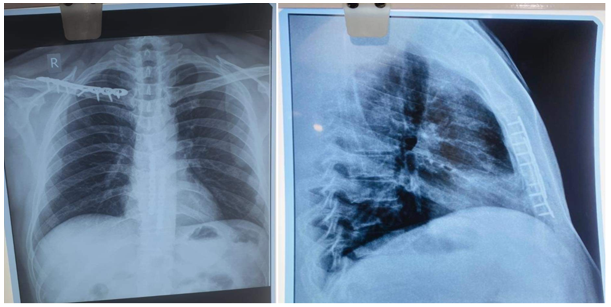
1 year Post op images
X
![]()
1 year Post op clinical images
X
![]()
Case 2
- Case of a 48-year-old male patient
- Polytrauma after fall from height
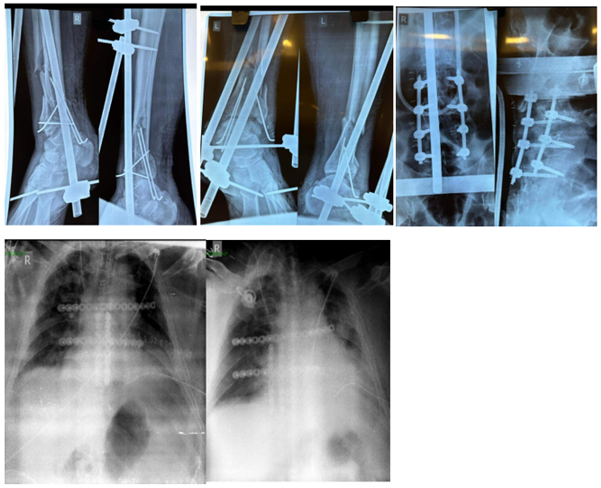
- Sustained bilateral grade 3 B severely communited open fracture of distal tibia and fibula with anterior wedge collapse fracture of L4 vertebrae with multiple bilateral ribs fracture (flail chest) with sternum fracture
- He also had co- morbidities like uncontrolled DM and morbid obesity.
- He was operated in a staged manner.
- In 1st stage bilateral ankle spanning external fixators were applied.
- Patient was in the ICU on ventilator for quite a long time, but ICU team was unable to extubate the patient due to flail chest.
- So stage 2 operation was planned in which bilateral ribs and sternum were fixed with multiple plates and screws.
- After this, ICU team managed to successfully extubate the patient.
- In stage 3, L4 collapse fracture was fixed using minimally invasive surgery.
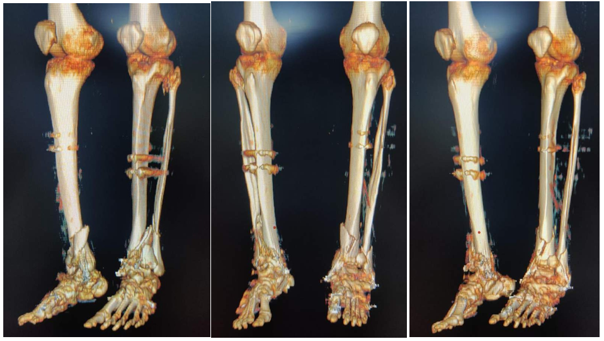
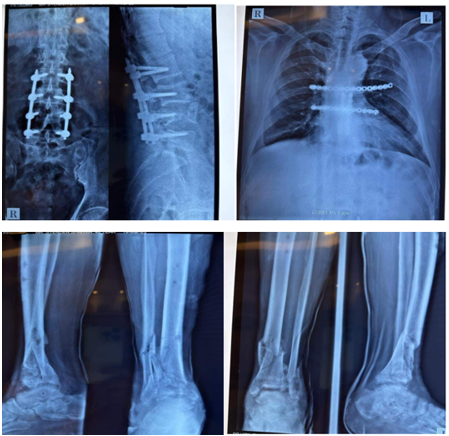
Pre op x-rays showing severely comminuted bilateral distal tibia and fibula fracture
X
![]()
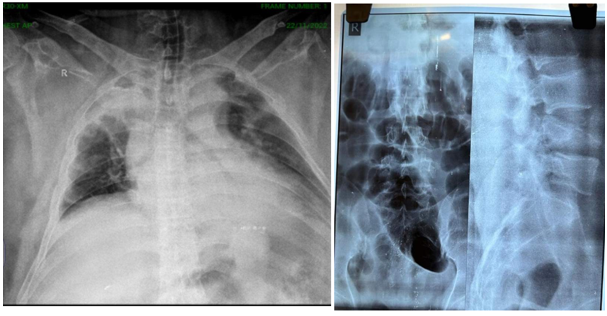
Pre op x-rays showing L4 anterior wedge collapse fracture with Bilateral multiple ribs fracture
X
![]()
Pre op clinical images
X
![]()
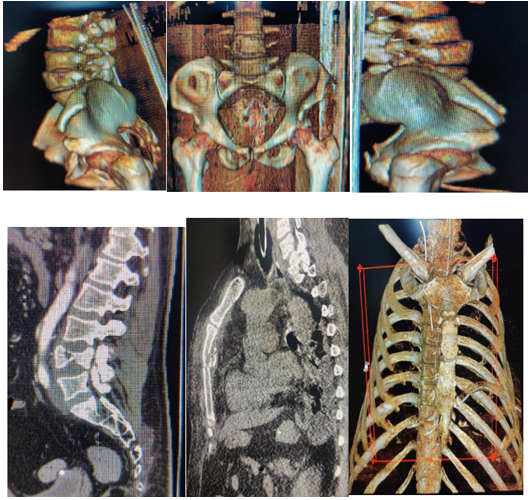
Pre op CT scan images
X
![]()
Pre op CT scan images
X
![]()
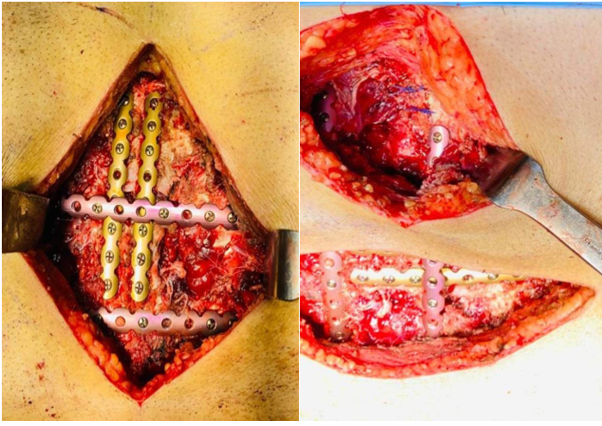
Intra op images
X
![]()
Immediate post op x-rays
X
![]()
Post op clinical image
X
![]()
3 months post op check x-ra
X
![]()
1 year post op X rays
X
![]()
1 year post op clinical images
X
![]()
Case 3
- Case of 46yr old male
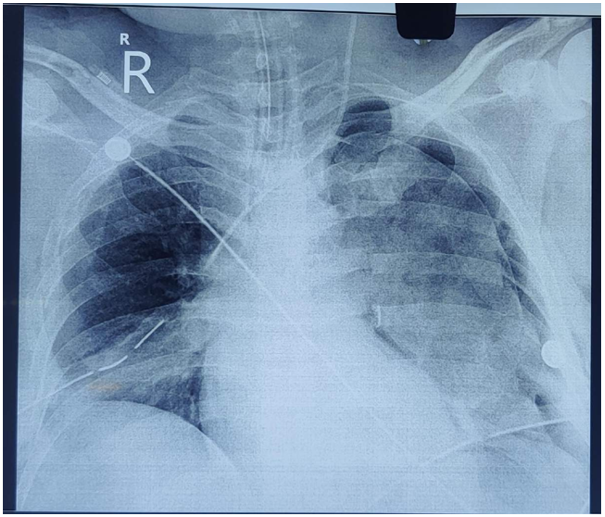
- RTA (polytrauma)sustaining multiple ribs fracture with hemothorax on left side, pneumothorax on rt side with surgical emphysema, in sepsis.
- He also has comorbidities like uncontrolled Diabetes with morbid
- Initially he was managed with bilateral chest tube insertion and epidural catheterization for pain
- However later on he developed bradycardia, hypotension, unresponsive for which he required three times CPR to revive
- He was subsequently
- And now the ICU team and primary team was in dilemma as patient could not be extubated because of flail chest, as he has multiple segmental displaced ribs fracture pushing into his lung parenchyma causing every now and then lung to completely collapse requiring urgent bronchoscopy at times. Hence we were called upon , we got fresh chest x Ray’s and CT chest to assess the patient’s status
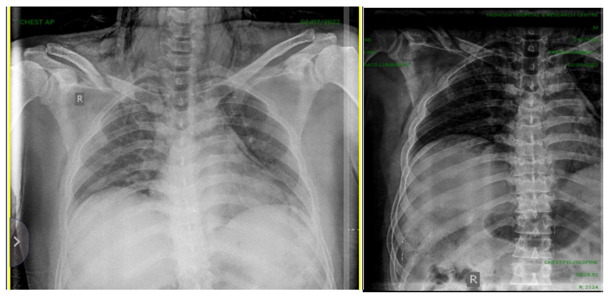
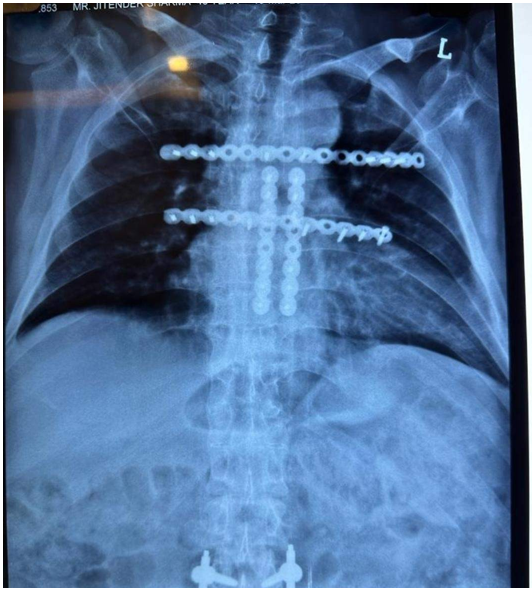
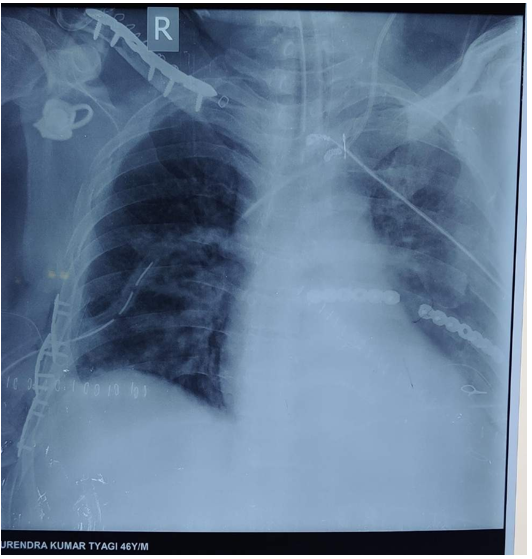
Pre op x-ray showing multiple ribs fracture bilaterally
X
![]()
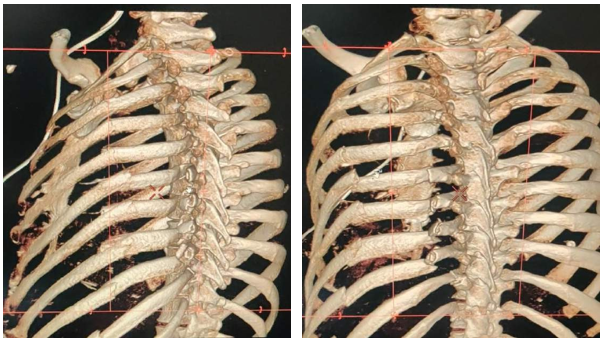
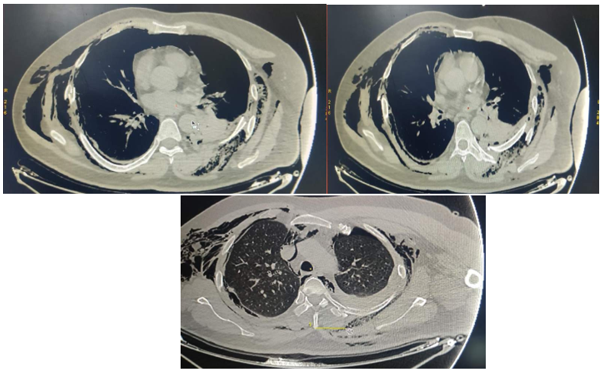
NCCT chest showing multiple ribs fracture at the level of angle on right side
- Right side-1st to 7th ribs were fracture along with clavicle fracture.
- Lateral end clavicle fracture
- 1st rib- undisplaced fracture
- 2nd rib-displaced fracture
- 3rd rib- displaced fracture
- 4th rib- segmental undisplaced fracture
- 5th rib- mild displaced fracture
- 6th rib- mild displaced fracture
- 7th rib- displaced fracture
X
![]()
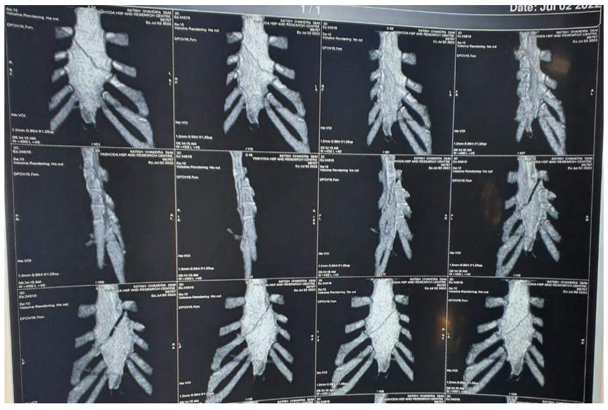
NCCT chest showing multiple segmental ribs fracture on left side
- Left side-1st to 10th rib fractures
- 1st rib - head fracture
- 2nd rib- head undisplaced fracture
- 3rd rib - mild displaced segmental fracture
- 4th rib-displaced segmental (3 fractures)
- 5th rib displaced segmental fracture
- 6th rib - displaced segmental fracture
- 7th rib segmental displaced fracture
- 8th rib- segmental displaced fracture
- 9th rib segmental displaced fracture
- 10th rib-displaced fracture
X
![]()
Pre op planning
- After thorough planning and taking high risk informed consent, patient was planned for operation.
- Right side-distance from spinous process to fractured angle of rib
- 4th rib proximal- 6cm and Distal- 13cm
- 5th rib- 15cm
- 6th rib - 18cm
- 7th rib-15cm
Pre op planning
- Left side - distance from spinous process to proximal and distal fracture of the ribp
- 4th rib - proximal fracture- 5cm and Distal fracture -12cm (straight distance), 15cm (curved distance)
- 5th rib- proximal fracture- 4cm and Distal fracture- 12cm, 16cm
- 6th rib- proximal fracture- 6cm and Distal fracture - 11cm, 14cm
- 7th rib- proximal fracture - 5.5cm and Distal fracture - 11cm, 14cm
- 8th rib-proximal fracture - 6cm and Distal fracture -11cm, 14cm
Pre op CT scans
X
![]()
Operative procedure
Following operative procedure was done-
- ORIF of 3 segmental left side rib fracture with S. wires, plates and screws
- ORIF of 3 right side rib fracture at level of angle with plates and
- ORIF of fracture lateral end of clavicle with plate and screws
X
![]()
Immediate post op x-rays
X
![]()
Post op clinical images
X
![]()
Result
- Of the 10 patients operated three were excluded due to lost to follow
- Of the 7 patients included in the study, all the patients were on ventilator pre-operatively and 24h post-operatively.
- The mechanism of injury was in 80% of cases either traffic accidents (60%) or falls (20%). The indication for surgery was failure to extubate due to flail chest in all the patients
- The included patients consisted of 6(60%) men and 4 (40%) women with the mean age of 57 years (20-86), mean Injury Severity Score (ISS) 48.1 (32- 63).
- 70% of the included patients in our study attended each follow-up.
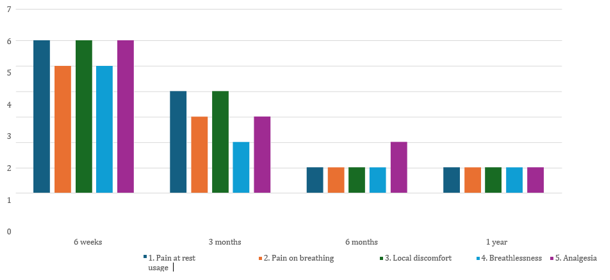
- The proportion of patients seen at follow-up with pain at rest and local discomfort decreased from 85.7% to 14.2% between 6 weeks and 1 year after surgery with standard deviation of 2.12 (30.33%).
- Problems associated with pain on breathing and breathlessness decreased progressively from 71.4% to14.2% at the end of 1 year with standard deviation of 1.63 (23.44%)
- Despite enduring pain, there was a significant decrease in the proportion of patients using analgesia from 85.7% to 14.2% after 1 year with standard deviation of 1.87 (26.75%).
Health related- Quality of life (EQ-5D-3 L questionnaire)
Proportion of patients at follow-up with subjective symptoms after rib fracture surgery
X
![]()
X
![]()
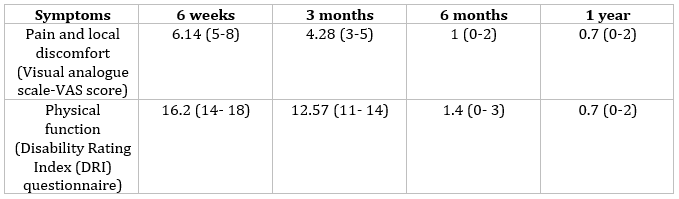
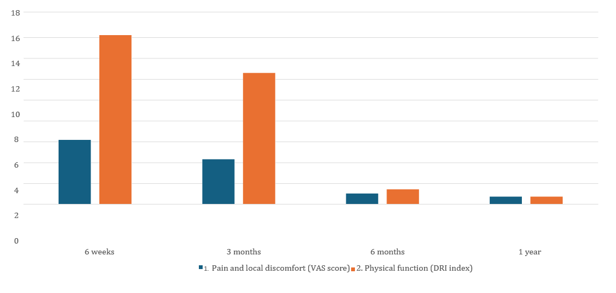
- The pain and local discomfort measured by Visual Analogue Scale (VAS) improved significantly over time: mean VAS was 6.14 (5-8) at 6 weeks, 4.28 (3-5) at 3 months, 1 (0-2) at 6 months and 0.7 (0-2) after 1 year with standard deviation of 2.27.
- Quality of life significantly increased between 6 weeks to 1 year following surgery.
- Physical function increased significantly over time.
- Mean Disability rating index was 16.2 (14-18) at 6 weeks, 12.57 (11-14) at 3 months, 1.4 (0-3) at 6 months and 0.7 (02) at the end of 1 year with standard deviation of 6.8.
Overall outcome
Proportion of patients at follow-up showing their VAS score and DRI Index after rib fracture surgery
X
![]()
X
![]()
Discussion
- In this study of 10 trauma patients who underwent stabilizing surgery of rib fractures, we found progressive improvement in pain, physical function and quality of life during the first, post operative year.
- The primary end-point in previous studies of surgical treatment of flail chest has mainly focused on aspects associated with respiratory insufficiency. Although acute pain can contribute to respiratory problems, chronic pain can be debilitating and lead to decreased Quality of life.
- It is probable that surgery decreases chronic pain. In the prospective RCT of Tanaka., et al., symptoms of chest tightness, thoracic cage pain and dyspnea on effort were more frequent in conservatively-managed patients.
- Surgery per se is associated with morbidity, however, and few of our patients experienced some form of local discomfort, although it was unclear whether this was due to the trauma or surgery.
- Despite enduring pain and discomfort, few of patients used analgesics, suggesting mild and not particularly disabling symptoms.
- Patients quality of life improved gradually after surgery, which is higher than that of a Swedish population study, which showed a mean VAS of 77.4 and 75.8% for men and women, respectively [13].
- Physical function, assessed by DRI, improved gradually and significantly with time.
- The results may also reflect long-term outcome of concomitant injuries; however, we found that few of trauma patients who have undergone surgical fixation of flail chest have no remaining disability after 1 year.
- Previous studies of conservatively-managed patients with flail chest have shown that 66 and 38% of them experienced persistent disability after 2 months and during a mean follow-up period of 5 years (6 months-12 years, respectively. Marasco., et al. found that 71% of conservatively managed patients experienced daily limitations and disabilities after 3 months compared to 48 of operated patients, suggesting that surgical management of flail chest decreases prolonged disability, although this may be particularly evident in cases of isolated thoracic injuries.
- The results of this study are limited as this was an uncontrolled study. The patients included were mostly subjected to polytrauma, as demonstrated by injury severity score.
- Poly-trauma patients are an inherent, heterogeneous group with associated injuries in addition to their thoracic trauma, which serve as confounding factors influencing the perception of pain, function, activity and QoL.
- Results from patients with isolated thoracic injury are likely to have been more homogenous and easier to interpret, but such a group would not have been representative of the population at large.
- Even in isolated thoracic injury, however, there are confounding factors due to commonly associated clavicle and scapular fractures that influence the mobility, function and pain of the thoracic cage. Moreover, the pre-existing pain, function and disability were unknown for patients in this study.
- Surgical treatment of rib fractures has received increasing attention in recent years. While previous studies have largely focused on the treatment of flail chest, it is not clearly defined if patients with multiple rib fractures or dislocated ribs also benefit from surgery.
- We chose to study the long-term results of patients with flail chest as this group has been the main focus of previous studies. However, patients with multiple rib fractures that required surgery for other reasons, were also stabilized and therefore included in this study.
- With the development of minimally invasive approaches to rib fixation more will be gained from surgery and the indications may well include multiple rib fractures in the future.
- A muscle-sparing approach to the ribs and a selective usage of thoracotomy would presumably decrease post-operative pain. However, muscle-sparing techniques minimize access to the injured chest wall making it difficult to fixate multiple rib fractures.
- Video-assisted thoracoscopic surgery (VATS) could be used to clear out hematoma and resect leaking lung tissue. However, the technique does require lung deflation to some extent, which may not be possible in all trauma patients with severe lung contusions.
- There is a need for larger prospective RCTs that compare not only the outcome of surgery concerning ventilator support and Intensive Care Unit (ICU) care, but also the long term outcomes associated with pain, function, activity and QoL, as well as cost-benefit of such surgical management.
Conclusion
Patients who underwent surgical plate fixation of multiple rib fractures and flail chest (on ventilatory support) showed a gradual improvement in symptoms associated with pain, physical function and Quality of life which continued Throughout the first post- operative year.
Bibliography
- Ziegler DW and Agarwal NN. “The morbidity and mortality of rib fractures”. Journal of Trauma 6 (1994): 975-979.
- Gennarelli TA., et al. “Association for the Advancement of Automotive Medicine”. The Abbreviated Injury Scale 2005 - Update (2008).
- Fabricant L., et al. “Prolonged pain and disability are common after rib fractures”. The American Journal of Surgery 5 (2013): 511-515.
- Landercasper J., et al. “Long-term disability after flail chest injury”. Journal of Trauma 5 (1984): 410-414.
- Bemelman M., et al. “Historic overview of treatment techniques for rib fractures and flail chest”. European Journal of Trauma and Emergency Surgery 5 (2010): 407-415.
- Tanaka H., et al. “Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients”. Journal of Trauma 4 (2002): 727-732.
- Granetzny A., et al. “Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status”. Interdisciplinary CardioVascular and Thoracic Surgery 6 (2005): 583-587.
- Marasco SF., et al. “Prospective randomized controlled trial of operative rib fixation in traumatic flail chest”. Journal of the American College of Surgeons 5 (2013): 924-932.
- Granhed HP and Pazooki D. “A feasibility study of 60 consecutive patients operated for unstable thoracic cage”. Journal of Trauma Management and Outcomes 8.1 (2014): 20.
- Fagevik Olsén M., et al. “Recovery after stabilising surgery for “flail chest”. European Journal of Trauma and Emergency Surgery 5 (2013): 501-506.
- Group TE. “EuroQol-a new facility for the measurement of health-related quality of life”. Health Policy3 (1990): 199208.
- Salén B., et al. “The Disability Rating Index: an instrument for the assessment of disability in clinical settings”. Journal of Clinical Epidemiology 47 (1994): 1423-1435.
- Burstrom K., et al. “Deteriorating health status in Stockholm 1998-2002: results from repeated population surveys using the EQ-5D”. Quality of Life Research 9 (2007): 1547-1553.










 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License







