Moutei Hassan*, Bennis Ahmed, Fouad Chraibi, Meriem Abdellaoui and Driss Benatiya
Ophthalmology Department, Faculty of Medicine and Pharmacy of Fez, Morocco
*Corresponding Author: Moutei Hassan, Ophthalmology Department, Faculty of Medicine and Pharmacy of Fez, Morocco.
Received: January 22, 2021; Published: March 19, 2021
Citation: Moutei Hassan., et al. “Improving Access to Healthcare Via Telemedicine in Ophthalmology: A Cross-sectional Study”. Acta Scientific Ophthalmology 4.4 (2021): 216-222.
Objective: The aim of this study was to Analyze the direct and indirect impact of the conventional health care system and compare it to the telemedicine-assisted system and to evaluate patient satisfaction.
Conception: This was a cross-sectional study conducted in the ophthalmology department at the Missour Provincial Hospital in collaboration with the Hassan II University Hospital Center in Fez.
Methods: A satisfaction investigation was conducted over a 30-day inclusion period. Data were collected through a questionnaire. The questionnaire was given to each patient at the end of the teleconsultation if they agreed to participate in the study. The EVA scale was used to determine global patient satisfaction. Very satisfied patients were rated 8-10, moderately satisfied 4-7, and dissatisfied 0-3.
Results: A total of 35 patients were included in the study. Participants were predominantly female (n = 21, 60%). The mean age was 61 years. There were 47 requests out of a total of 200 patients who had consulted during this period: 40 requests were referred for a complementary examination and 8 for a specialized consultation. From the patients' point of view, the 47 requests for additional examinations and specialized consultations for 35 patients had resulted in direct savings equal to 13,090 MAD (1190 Euro) for 1 month. In addition, doctors had succeeded in improving the speed of patient care and, at the same time, reducing the need for secondary care, with 97% overall satisfaction. However, 100% of practitioner users were satisfied with the tool and found it easy to use. They found the tool to be a major help in times of health crisis (COVID-19).
Conclusion: Telemedicine is particularly important for Morocco considering its vast geographical area and predominantly rural population where medical care was not widely available and sometimes not easily accessible. The deficit in numbers of doctors, both general practitioners and specialists, necessitated the development of new forms of practice. Telemedicine gave rise to the expectation of better coverage of distant areas by offering second-line care. Morocco was lagging behind the Anglo-Saxon and Scandinavian countries, where telemedicine had already been part of their practice for some twenty years.
Keywords: Teleophthalmology; Telemedicine; Healthcare
Ophthalmology is a medical specialty that could benefit from telemedicine and teleophthalmology services. These services were very important in poor, remote and impassable geographical areas, where there was no access to ophthalmology services. National health systems were faced with the challenge of providing better quality health care. However, in the face of the low medical demographics in some regions of Morocco, including the Boulemane region, telemedicine was presented as a promising solution.
In addition to its contribution to improving the quality of healthcare provision, telemedicine could also resolve territorial health inequalities. Urban, rural and semi-rural residents would thus benefit from an equitable offer of care [1]. Telemedicine is particularly important for Morocco considering it’s vast geographical area and predominantly rural population where medical care was not widely available and sometimes not easily accessible. The deficit in numbers of doctors, both general practitioners and specialists, necessitated the development of new forms of practice. Telemedicine gave rise to the expectation of better coverage of distant areas by offering second-line care. Morocco was lagging behind the Anglo-Saxon and Scandinavian countries, where telemedicine had already been part of their practice for some twenty years [2].
The aim of this study was to Analyze the direct and indirect impact of the conventional health care system and compare it to the telemedicine-assisted system and to evaluate patient satisfaction.
This was a cross-sectional study conducted in the ophthalmology department at the Missour Provincial Hospital in collaboration with the Hassan II University Hospital Center in Fez.
The Hassan II University Hospital of Fez It is the largest of the five university hospitals in terms of size, litter capacity and even in terms of the diversity of the specialties it houses, both medical and surgical.
The activity of the ophthalmology department at the Hassan II University Hospital concentrates mainly on consultations (800 patients/month). Surgical operations constitute the second important part of the department's activities. They can be performed on ambulatory patients (600/month) or on hospitalized patients when the family situation, geographical location or medical reasons require it. The Ophthalmology Department can manage and treat all ocular pathologies. The team is composed of 4 professors, about 30 resident doctors, 5 orthoptists. Finally, an administrative and nursing team assures the secretariat, the reception of patients and some technical acts.
The Hassan II University Hospital Center assures the provision of care in the Fez-Boulmane region. This region is actually composed of 03 provinces and 01 prefecture:
The region of Fez Boulemane covers an area of 20,435.86 km², divided between the provinces of Sefrou (19.62%), Boulemane (70.44%) and My yacoub (8.32%) and the prefecture of Fez (1.62%). It includes 12 urban communes and 48 rural communes (Figure 1).
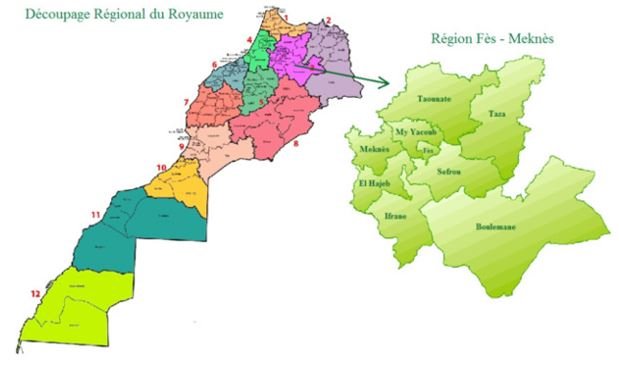
Figure 1: Regional division of the Kingdom of Morocco [3].
The region has a population estimated at 1,852,000 (year 2012) with a high concentration in the prefecture of Fez (1,149,000 inhabitants), followed by the province of Sefrou (270,000 inhabitants), the province of My Yaacoub (232,000 inhabitants) and finally the province of Boulemane (201,000 inhabitants).
Le circuit initial du patientAfter the initial visit of the patient to the Missour Provincial Hospital for an ophthalmologic consultation, additional test was sometimes required, such as: optical coherence tomography, retinal angiography, corneal topography... or a specialized advice (corneal consultation, glaucoma consultation, retinal consultation...). In this situation, the patient was obliged to go to the nearest ophthalmology reference center in Fez (Hassan II University Hospital in Fez), about 199 kilometers away (the trip by car lasted 3 hours and 06 minutes (one way). The first trip was only to book an appointment for a care service, the second trip was to benefit from the care service requested by the doctor, and the third trip was to obtain the results of the complementary examinations. All of these trips were stressful for the patient (Figure 2).
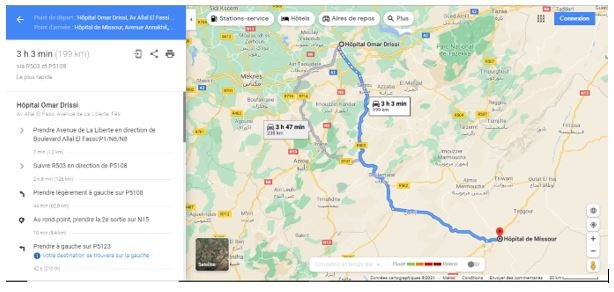
Figure 1: The trip between the provincial hospital " green walk " and the ophthalmology department of the Hassan II University Hospital Center of Fez (google maps).
The system for remote appointment schedulingThe remote appointment scheduling system plays an important role on the patient's point of view. When it was designed and deployed based on the patient's needs and wishes, it helped providers better understand patient problems, identify system weaknesses, increase patient satisfaction and improve clinical outcomes.
The appointment scheduling system was realized via the "HOZIX" platform. It was an easy-to-use system that health professionals could access on the HOZIX application. The telemedicine platform was secure and approved for hosting health data. Doctors also did not require a high-performance computer; users could use any computer with a web browser: laptop/notebook, cell phone or desktop computer. The system provided the platform to facilitate the booking and management of patient appointment bookings. Doctors could also view reports of requested additional tests. It was necessary for each new patient to register before being able to access the system, each patient needed to have an identifier that they could use to log on before they could book an appointment for a further examination or specialist consultation. The doctor could also print the appointment as a confirmation document.
The protocolA satisfaction investigation was conducted over a 30-day inclusion period. All patients participated voluntarily, and the data they contributed to this study would remain confidential. Data were collected through a questionnaire. Patients who did not fully complete the questionnaire or did not wish to participate in this study were excluded from the study.
The questionnaire was given to each patient at the end of the teleconsultation if they agreed to participate in the study. In the absence of a validated questionnaire, we developed a self-designed questionnaire based on the two references [2,4]. The questionnaire was divided into three sections as follows: patient demographics, satisfaction information, and appointment scheduling information.
The values presented correspond to counts (proportions) for categorical variables and means [± standard deviation] for quantitative variables.
All patients had signed a consent form. The study was conducted in accordance with the principles of the Declaration of Helsinki.
A total of 35 patients were included in the study. Participants were predominantly female (n = 21, 60%). The mean age was 61 years. However, the age distribution was heterogeneous: 17.14% of patients were under 40 years of age, 28.57% of patients were between 40 and 60 years of age, while 54.28% of patients were over 60 years of age. A total of 10 (28.57%) patients were active. However, most of the patients 25 (71.42%) were retired and housewives (Table 1).
|
Study Population (n = 35) |
n (%) |
|
Age <40 years 40-60 years >60 years Sex Man Woman Location Active Not working (retired, housewife, unemployed) |
6(17,14%) 10(28,57%) 19(54,28%)
21 (60%) 14(35%)
10(28,57%) 25(71,42%) |
Table 1: Comparison of clinical characteristics between the stenting and emergency surgery groups.
ASA – American Society of Anesthesiologists.
Data are expressed as mean (SD) or absolute number of patients (%).
Table 2 presents the various complementary examinations and specialized consultations requested at the Missour Provincial Hospital. There were 47 requests out of a total of 200 patients who had consulted during this period: 40 requests were referred for a complementary examination and 8 for a specialized consultation (Table 2).
|
Study Population (n=35) |
n (%) |
|
Additional examinations Macular optical coherence tomography Papillary optical coherence tomography with ganglion cell counting Retinal angiography Corneal topography Specular microscopy Specialized consultation Corneal consultation Retinal Consultation Glaucoma consultation Pediatric Consultation |
15(31,91%) 3(6,38%)
12(25,53%) 6(12,76%) 4(8,51%)
3(6,38%) 1(2,12%) 2(4,25%) 1(2,12%) |
Table 2: Characteristics of the various complementary examinations and specialized consultations requested.
The distance between health structuresThe average distance between the provincial hospital center and the nearest university hospital center, where patients could benefit from complementary examinations and specialized consultations was 199km, which corresponded to a 3-hour 06-minute one-way trip. In addition, the distance between the provincial hospital center and the patient's place of residence was classified into 3 categories: 25.71% of patients lived within 50 km of the hospital, 45.71% between 50 and 100 km and 28.75% over 100 km. This corresponded to an average of 60.5 min one way trip (Table 3).
|
199km / 3heure 06 minutes
117km / 1heure 40 minutes
61km / 55minutes
41km / 41 minutes
49 km / 46 minutes |
17 Euro
10 Euro
6 Euro
4 Euro
4 Euro |
Table 3: The distance between the provincial hospital and the teaching hospital center and the areas served by the provincial hospital.
Since this optimistic scenario is based on the assumption of easy access to the hospital and did not take into account common contingencies (e.g., traffic, meteorology especially in winter, actual distance....).
Organizational impactThe main advantage of teleophthalmology was a reduction in the number and cost of patient travel, with a consequent improvement in quality of life. In addition, doctors had succeeded in improving the speed of patient care and, at the same time, reducing the need for secondary care, with 97% overall satisfaction.
Table 4 Whereas, the introduction of additional staff, such as nurses or assistants, could improve service.
|
|
Score |
Results |
|
Timeliness of care Saving on the number of trips Savings in financial expenses |
1-10 1-10 1-10 |
8,1 9.8 9.7 |
Table 4: Organizational Benefits.
From the patients' point of view, the 47 requests for additional examinations and specialized consultations for 35 patients had resulted in direct savings equal to 13,090 MAD (1190 Euro) for 1 month. In particular, they were saved through the avoided trips to make an appointment on site at the CHU the first time (17 Euro per person for a round trip by public transport from the green walk hospital to the Hassan II CHU) and the recuperation of the interpretation of the complementary exams the second time (the same cost for a round trip). Thus, the equivalent of 34 Euro per person in total, not counting in some situations the trip between the patient's accommodation and the provincial hospital of Missour.
Practitioners100% of practitioner users were satisfied with the tool and found it easy to use. They found the tool to be a major help in times of health crisis (COVID-19).
In recent years, computer and communication systems have been developed and applied to various health care areas. Using this technology, health care services had evolved to become more accessible and efficient, especially when distance was a major preoccupation (such as in our study). In fact, to overcome geographical disparities in health, telemedicine became a discipline to improve health services around the world.
Ophthalmology was a medical specialty that could benefit from telemedicine and teleophthalmology services. These services were very important in poor, isolated and impassable geographical areas, where there was no access to various ophthalmological explorations. In these areas, due to the prevalence of eye diseases and limited access to medical equipment, patients could suffer from low vision or blindness. The use of this technology could facilitate the diagnosis and management of eye diseases [5]. In our study, 54.28% of the patients were over 60 years of age, making it very difficult for this age group to travel many times to the university hospital center. However, 10 (28.57%) patients were active, which may affect their productivity.
The use of telemedicine services in the specialty of ophthalmology could also help to increase the speed and quality of eye care services and could reduce unnecessary and time-consuming visits across the country. Telemedicine was well received when imaging was at the heart of the system. The rapid transmission of data and images was one of the most important aspects of tele-ophthalmology that allowed physicians to consult and make decisions very quickly. This, in turn, could improve the quality of patient care, especially in isolated areas.
Many studies had shown that patients were satisfied with the way health care was provided through telemedicine [6]. Various satisfaction surveys in teleophthalmology reported a good level of satisfaction, but most of them were limited by a smaller sample size. Overall satisfaction with remote patient appointment scheduling was excellent with 97% of patients satisfied or very satisfied in this study. We are aware that this study was one of the first surveys to evaluate patient satisfaction with the appointment scheduling systems for the performance of complementary exams and/or specialized consultation at the UHC from a provincial hospital.
Indeed, the deficit in ophthalmologic exploration devices in these territories forces doctors to refer their patients to neighboring CHU hospitals some 100 kilometers away. Thus, appointment delays were long and the iterative movement of patients seems inevitable. Telemedicine would be a miraculous solution to this lack of infrastructure. The main advantages attributed to telemedicine were facility of access to second recourse, reduction of costs, reduction of unnecessary referrals to specialists, reduction of unnecessary travel and development of efficient communication between doctors in different sectors. Telemedicine also made it possible to monitor pathologies usually managed at the referral center such as macular edema, age-related macular degeneration, etc. (at a distance from the acute phase).
For healthcare professionals, the online appointment scheduling platforms offered time savings and efficiency in the management. Users also appreciated the practicality and speed of the service when they needed an additional examination or specialist advice. The online availability of the results of additional examinations made it easier for the requesting doctor, avoiding the need for the patient to travel to retrieve the report and eliminating the need for repetitive analyses and tests. Sometimes, several disciplines could be engaged for a single patient. A central database of patient health records will allow various medical personnel to interact on a common platform and facilitate therapeutic decision making.
However, failure to keep appointments due to the difficulty of repeated travel and remoteness could result in loss of income and disruption of workflow. When a patient missed a scheduled appointment, the hospital did not receive payment for that time slot. On average, a medical facility would have a non-attendance rate of about 14%. This could result in a significant loss of revenue that could range from 3 to 14% [7]. Online appointment scheduling systems significantly reduced absences, since the patient would only have to travel once, thus reducing expenses, although it would eliminate overbooking, which could lead to patient dissatisfaction due to extended appointment times.
In addition, paper usage could be reduced to a large extent with online systems. This was more relevant in today's world, reducing the impact on the environment. Paper consumption had decreased in recent years with the greater availability of large-screen portable devices that could be used to access and display information. In addition, paper would mean files, cabinets, shelves, which required cleaning and maintenance.
Health providers were turning to technology to update and improve the quality of their services. Online appointment scheduling systems were definitely a step forward for these medical service providers. Eliminate the hassle of appointment management; make workflow less cluttered; improve data entry and communication; save time; provide patients with more choice and convenience, improving patient confidence and loyalty. All of these benefits were the reason for adopting a remote appointment scheduling system in a primary care hospital.
“The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper”.
No funding was allocated to this study.
Copyright: © 2021 Moutei Hassan., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff