KKrishna Kumar1* and VJ Niranjana Bharathi2
1Senior Consultant, Apollo Speciality Hospitals, OMR, India
2Junior Consultant, Apollo Speciality Hospitals, OMR, India
*Corresponding Author: K Krishna Kumar, Senior Consultant, Department of Otorhinolaryngology, Apollo Speciality Hospitals, OMR, India.
Received: May 13, 2021; Published: May 26, 2021;
An upper airway obstruction secondary to a subglottic tumor can be easily misdiagnosed as bronchial asthma. We report a 16 year old girl who was misdiagnosed as bronchial asthma whereas finally diagnosed as spindle cell lesion of subglottis. The challenging feature of head and neck pathology is a varied array of spindle cell lesions ranging from reactive to malignant and very aggressive. Hence an accurate diagnosis is critical which can be obtained with the help of diagnostic and radiological facilities.
Keywords: Subglottic Mass; Spindle Cell Lesion
Spindle cell lesions seen in the head and neck region have a varied diversity. They are rare tumors which could be malignant, benign or just reactive lesions. These lesions can occur at varied regions like head and neck skin, scalp soft tissues, soft tissues of neck, upper aerodigestive tract mucosa, etc. The most commonly seen lesion is the spindle cell carcinoma which is a highly malignant variant. Hence it has to be ruled out before diagnosing the benign or reactive lesions. The features of the spindle cell tumor can mimic various reactive, benign, and malignant lesions[1] (Table 1). Hence the diagnosis is very challenging.
| Malignant | Benign or low grade | Non-neoplastic |
|---|---|---|
Spindle cell carcinomaa |
Nodular fasciitis |
Sinonasal polyp with stromal atypiaa |
Spindle cell melanoma |
Glomangiopericytoma |
Ulcer with granulation tissue/radiation-induced atypiaa |
Spindle cell myoepithelioma or carcinoma |
Inflammatory myofibroblastictumora |
Vocal cord nodule with stromal atypiaa |
Kaposi’s sarcoma |
Solitary fibrous tumor |
Contact ulcera |
Other sarcomas: angiosarcoma, synovial sarcoma, MPNST |
Ossifying and non-ossifying fibroma |
Giant cell fibroma |
Table 1:Differential diagnosis for spindle cell lesions presenting at UADT mucosal sites.
A 16 year old girl was referred to us by our pulmonologist with complaints of shortness of breath. She was being treated as bronchial asthma for the past 2 years elsewhere with no improvement in the quality or ease of breathing. There was no hoarseness of voice, loss of weight or appetite. There was no odynophagia nor dysphagia. The routine ENT examination was normal. Hence a video laryngoscopy and diagnostic nasal endoscopy was done. Video laryngoscopy(Figure 1) revealed a linear diffuse mass just below the vocal cords in the subglottis with airway narrowing. Bilaterally the vocal cords were normal and mobile. CECT Neck(Figure 2) was done which revealed a gross asymmetric soft tissue thickening of both vocal cords (Rt > Lt) with 80% luminal narrowing and mild heterogeneous post contrast enhancement which was likely to be infective in origin. Patient was then taken up for Tracheostomy due to very narrow airway followed by Microlaryngealcoblation excision of the entire subglottic mass. The histopathology showed features consistent with a spindle cell lesion with no mitosis or necrosis. It was followed by IHC which showed positivity in Vimentin and SMA. CK, S100, CD34, BetacateninandDesmin were negative. The final result was suggestive of Spindle cell proliferation which is probably reactive. Patient was decannulated within a month of surgery. She was followed up for 6 months and there was a definitive improvement in the quality of breathing. There was no subsequent growth of lesion.

Figure 1:Figure 1
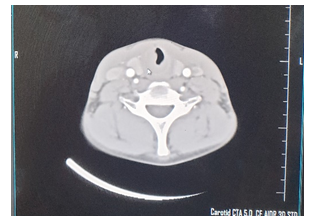
Figure 2:Figure 2
Though Spindle cell lesions presenting at the upper aerodigestive tract mucosal sites are usually straight forward to diagnose, there are a few lesions which are quite difficult to classify. With a proper history taking, clinical examination, radiological and histopathological examination with a judicious use of immunostains, one can work through these difficult cases. Though there are not many absolute features, there are several important points that could strongly favor malignancy. The features favouring malignancy or true neoplasia can be observed when we take deeper levels on small biopsies. A spindle cell lesion strongly favours malignancy if has features such as invasive growth at the periphery, areas of dense cellularity, well-formed fascicles, dense collagenous background, marked nuclear hyperchromasia in individual cells, etc.
Benign lesions usually show features such as zonation or true organization especially of vessels in the lesion, widely scattered nuclear atypia, lesional cells have vesicular chromatin with small nucleoli and lack mitotic activity. Spindle cell carcinoma lacking mitotic activity is very rarely observed[2]. They are usually highly mitotically active lesions.
In our case, it was a smooth surfaced lesion with absolutely no mitosis or necrosis. All features favoured a non-neoplastic lesion. There are not many benign cases reported in literature which makes this case presentation rare. A case was reported in the Archives of Otolaryngology and Rhinology by Sumana CV., etal. [3] which was also initially mistreated as Bronchial Asthma. A case similar to our case was reported by NurdanKorturk., etal. in The Journal of Emergency Medicine in 2004[4]. This shows that not all cases of wheeze can be taken as only asthma.
This case report emphasizes on the importance of a complete clinical examination with involvement of other specialities in the diagnosis. Though shortness of breath is not a typical ENT symptom, in this case it showed ENT pathology, Spindle cell lesion of subglottis. As spindle cell carcinoma is the most common lesion seen along the upper aerodigestive tract, it has to be ruled out before concluding on a less common lesion. This can positively be achieved by a very careful clinical examination, endoscopic examination, radiological and histopathological analysis which all go hand in hand. Thus, a collaborative analysis will lead us to a proper diagnosis and treatment.
Citation: K Krishna Kumar and VJ Niranjana Bharathi. “Rare Case of Benign Spindle Cell Lesion in Subglottis". Acta Scientific Otolaryngology 3.6 (2021):98-100 .
Copyright: © 2021 K Krishna Kumar and VJ Niranjana Bharathi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
