RamakrishnaBethanabatla* and Ahmad Taha
Department of Neurosurgery, Southern District Health Board, New Zealand
*Corresponding Author: Ramakrishna Bethanabatla, Department of Neurosurgery, Southern District Health Board, New Zealand.
Received: April 27, 2021; Published: May 21, 2021;
Mycobacterium tuberculosis (MTB) intracranial tuberculomas are rare and account for approximately 1% of all cases. Central nervous system (CNS) involvementis a serious condition if not treated adequately. We present a case of a lady who presented with Headaches.
Keywords: Mycobacterium tuberculosis (MTB);Central Nervous System (CNS);Intracranial Tuberculoma
Mycobacterium tuberculosis (MTB) intracranial tuberculomas are rare and account for approximately 1% of all cases. Central nervous system (CNS) involvementis a serious condition if not treated adequately and clinically CNS MTBpresentation could be with meningitis, intracranial tuberculoma and spinal tuberculous arachnoiditis. In developed countries, meningitis due to reactivation of the disease is most common[1]. The risk factors of MTB infection include demographic factors like low socio-economic conditions, compromisedimmunity secondary to HIV or drugs,malnutrition, alcoholism and malignancies [2]. Clinical presentation is similar to any space occupying lesion in the brain with headaches, nausea, vomiting and neurological deficits, and can present in the absence of MTB symptoms in other parts of the body [3]. Usual presentation is with frontal or parietal lobe involvement, but could occur anywhere in the CNS and with multiple lesions. Initial stage CT without contrast may show low-density or isodense lesions with perilesional oedema, and contrasted images may show encapsulated isodense or hypodense lesions with peripheral ring enhancement (target lesions) [3]. CNS MTB treatment usually consists of four-drug regimen including rifampin, isoniazid,pyrazinamide, and ethambutol (RIPE) or rifampin, isoniazid, pyrazinamide with either fluoroquinolone or aminoglycoside, administered daily for a period of 12 - 18 months. Steroids should be used for the first 2 months as well [4].
A 58 year old female otherwise fit and well, presented with 3 week history of right sided headache and nausea, and no abnormal neurological findings on examination. There was no history of any preceding respiratory illness and no significant travel history. All admission blood inflammatory markers and cultures where negative. A CT scan of the headshowed a right parietalenhancing lesion with oedema, and anMRI scan was performed which showed a rim enhancing lesion with meningeal enhancement and diffusion restriction, and the differential diagnosis was between an cerebral abscess and high grade vs metastatic lesion. CT chest, abdomen and pelvis - Negative.
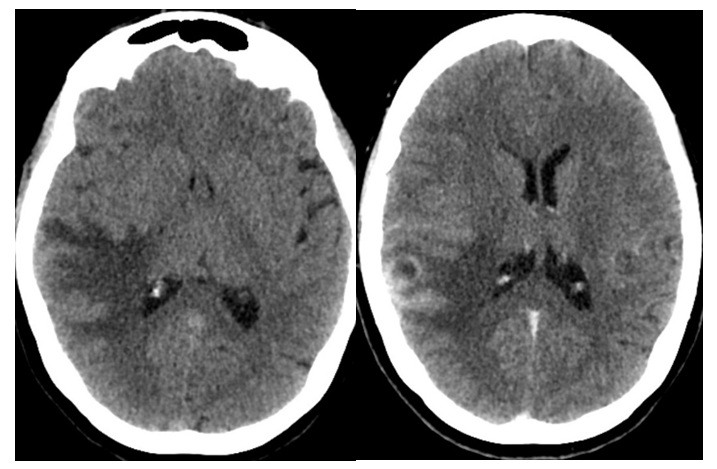
Figure 1:CT scan with and without contast.
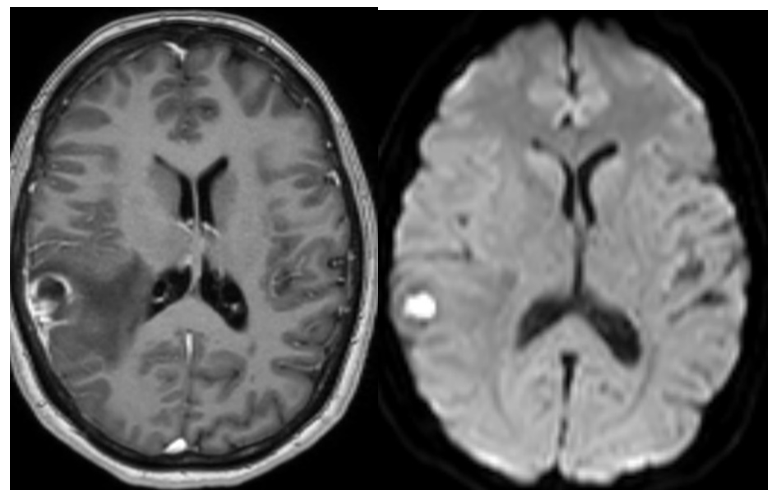
Figure 2:MRI with contrast and DWI sequences.
Patient underwent emergency craniotomy and excision of lesion with stealth guidance, intraoperatively the lesion was fibrous without any frank pus or thrombosed vessels and a thick capsule. Complete microscopic excision was performed without any post-operative complications.
The macroscopic pathological findings of specimen was a mass with a soft cheesy consistency and haemorrhage measuring 30 x 20 x 12 mm. Microscopic finding were brain with well circumscribed areas of necrosis, with peripheral histiocytes and mixed inflammation. Necrotising granulomata with multinucleated giant cells are present. Ziehl-Neelsen stain shows acid fast bacilli. Necrotising granulomatous inflammation- likely tuberculoma.
Although CNS TB is a rare disease in developed countries this should always be considered during differential diagnosis, and enquiry about patients exposure to TB or previous travel historyto endemic countries should be checked and documented at admission. In the absence of pulmonary disease, and in immunocompetent patients, symptoms and radiologic findings of CNS tuberculoma could be nonspecific and may be a clinical challenge to diagnose. CT imaging has been reported as having a sensitivity of 100% and specificity of 85.7% in CNS tuberculoma detection [5,8], in our case there were no suspicions raised of MTB tuberculoma. Brain magnetic resonance imaging (MRI) is the technique of choice for further investigation. Brain biopsy/excision of the lesion depending on the location is the most accurate method of diagnosis, especially in the absence of any other extra cranial manifestations[5]. Anti-TB drugs are the main stay of treatment of cerebral tuberculomas and should appropriately started once diagnosis is confirmed. This case illustrates the importance of havinghigh clinical suspicion for MTB, in immunocompetent patients and in non-endemic areas with history of exposure to a possible TB positive uncle at age 6.
Citation: Ramakrishna Bethanabatla and Ahmad Taha. “Intracranial Tuberculoma". Acta Scientific Otolaryngology 3.6 (2021):89-91 .
Copyright: © 2021 Ramakrishna Bethanabatla and Ahmad Taha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
