Rajesh C Kamble*, Alpana N Joshi and Pravin Mestry
Department of Radiology, Shobha Diagnostic Centre, Mumbai, India
*Corresponding Author: Rajesh C Kamble, Department of Radiology, Shobha Diagnostic Centre, Mumbai, India.
Received: March 08, 2021; Published: March 23, 2021
Vascular lesion is an all-encompassing term used to describe a wide range of conditions consisting of an abnormal number, structure, or position of blood vessels.
Keywords: Ultrasound; Vascular Lesions in Neck; Pediatric Vascular Neck Pathologies
Many classifications have been proposed, but to date a very basic classification system has been adopted by the International Society for the Study of Vascular Anomalies (ISSVA) [1]. This classification distinguishes two main types of vascular anomalies:
ISVA classification for vascular anomalies (Approved at the 20th ISSVA workshop, Melbourne, April 2014, last revision May 2018) [1].
|
Vascular anomalies |
||
|
Vascular tumours |
Vascular malformations |
|
|
· Benign · Locally aggressive or borderline · Malignant |
Simple |
Combined |
|
· Capillary · Lymphatic · Venous · Arteriovenous · Arteriovenous fistula |
· Capillary venous · Capillary lymphatic · Lymphovenous · Capillarylymphovenous · Capillary arteriovenous · Capillary lympho arteriovenous |
|
Table
Many vascular anomalies can be diagnosed by history and physical examination, making imaging unnecessary. However, when imaging is used, it is important to choose the modality based on the specific lesion and clinical situation [2].
Ultrasonography (US) and Magnetic resonance imaging (MRI) are the 2 most widely used modalities of choice [2].
All patient selected for this study were in pediatric age group of - 3 months of neonatal life to 7 - 8 years of age. The studies were performed on High end Philips - Affinity 70 system with high frequency linear transducers in range of 3 - 12 Mhz frequency. No sedation was used during these studies
US is used for initial screening because of its portability, lack of ionizing radiation, and no requirement of sedation in children. It is relatively simple, noninvasive, and yields good results for evaluating small, superficial and/or suspected, solid visceral lesions [2].
Typically, US is able to determine the basic type of lesion, direct initial management, and plan further imaging evaluation. Gray-scale B mode sonography, Color Doppler and spectral Doppler tracings are done to evaluate vascularity and determine types of vessels present [2].
MRI is helpful to further characterize sonographic findings and determine the extent of larger lesions for planning medical, interventional, and/or surgical therapy.
Between the two modalities, ultrasound is most preferred primary modality of choice all over the world.
Case no 1
Figure 1: Clinical picture.
USG images
Figure 2A
Figure 2B
Figure 2C
Figure 2D
Figure 2A-2D: 2A and 2B: B mode images showed echogenic mass situated in the subcutaneous soft tissues of the left neck. The mass showed few hypoechoic areas within it. 2C: On Colour Doppler, there is diffuse vascularity within the lesion suggestive of a vascular mass lesion. 2D: Spectral Doppler shows monophasic low velocity venous signal within it highly suggestive of a venous malformation.
USG diagnosisVenous vascular malformation.
DiscussionVascular malformations are true congenital lesions, which by definition are always present at birth, although they are not always detected [3].
Classification: Capillary, lymphatic, arterial, venous, or mixed. Vascular lesions have been categorized further into low- and high-flow types on the basis of the hemodynamic characteristics of the lesions, a distinction that is important in the choice of management strategies.
Clinical characteristics: Bluish, easily compressible, cold, and increase in size with valsalva maneuvers.
Gray-scale US: Hypo echoic, heterogeneous lesions in which phleboliths may be detected (pathognomonic if present), and they display compressibility [3,4].
At Doppler analysis, monophasic, low-velocity venous signal is encountered. The presence of slow arterial flow can suggest a mixed form of vascular malformation [3].
Case no 2
Figure 3A
Figure 3B
Figure 3C
Figure 3D
Figure 3A-3D: 3A and 3B shows normal homogenous appearance of the bilateral submandibular glands. 3C: Shows normal homogenous appearance of the left parotid gland. 3D: Shows heterogenous right parotid gland with hypoechoic spaces within them.
FI year old female child.
Figure 4: Heterogenous right parotid gland with phleboliths within.
Figure 5: Colour doppler shows diffuse vascularity within the right parotid gland.
Figure 6: Spectral doppler shows arterial flow within the lesion within the right parotid gland.
USG diagnosisParotid hemangioma.
Discussion
Figure 7A
Figure 7B
Figure 7C
Figure 7D
Figure 7A-7D: 7A-7C B mode USG images - Enlarged bulky right parotid gland. The gland appeared hypoechoic, heterogenous in echotexture with hyperechoic areas within it. 7D: Shows normal homogenous left parotid gland.
Figure 8A
Figure 8B
Figure 8A and 8B: Colour doppler shows increased vascularity within the heterogenous areas with chaotic vascularity pattern.
USG diagnosisWith above ultrasound appearance and history of rapid increase in the parotid swelling a diagnosis of parotid hemangioendothelioma was proposed. The pediatric surgeon excised the lesion and the histopathological diagnosis turned out the same.
Discussion
Figure 9A
Figure 9B
Figure 9C
Figure 9D
Figure 9A-9D: 9A and 9B: B mode ultrasound images showing normal homogenous appearance of the right and left parotid glands. 9C: Heterogenous lesion with few anechoic areas within seen at the angle of right mandible. The right submandibular gland was not seen separately from this lesion. 9D: B mode ultrasound image of left submandibular gland showing normal homogenous appearance.

Figure 10A
Figure 10B
Figure 10C
Figure 10D
Figure 10A-10D: 10A and 10B: Mode ultrasound image of the lesion at the angle of right mandible showing branching pattern of hypo/anechoic areas within. 10C and 10D: Colour doppler images of the lesion showing both arterial and venous signals within the lesion.
Figure 11A
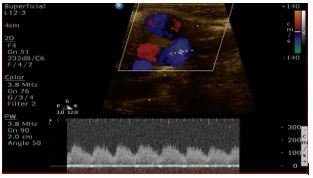
Figure 11B
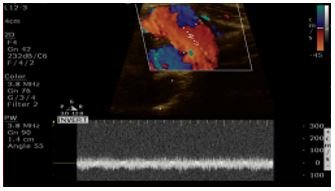
Figure 11C
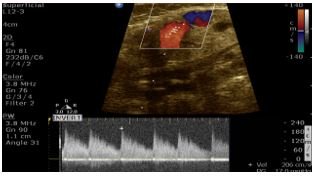
Figure 11D
Figure 11A-11D: 11A and 11B: Spectral colour doppler shows arterialized flow in the veins with velocity at 240 CM/SEC. 11C: Monophasic low velocity venous flow in some part of the lesion. 11D: Feeding artery to the lesion.
USG diagnosisRight submandibular arteriovenous malformation. Digital subtraction angiography confirmed our diagnosis with successful endovascular embolization done by the interventional radiologist.
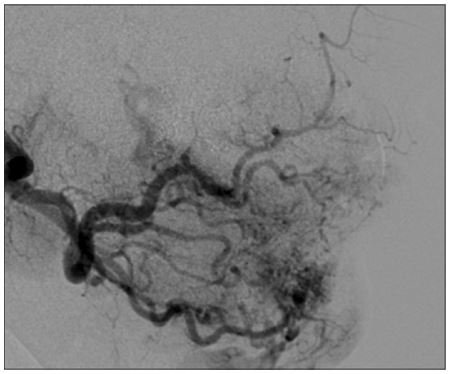
Figure 12: DSA of the lesion confirmed arterio- venous malformation of the right submandibular gland.
DSA of the lesion confirmed arterio- venous malformation of the right submandibular gland.
DiscussionThese cases highlight the fact that high frequency linear transducers have revolutionized the imaging of lesions in the neck. Ultrasound is a great tool to evaluate pediatric lesions in the neck as it is widely available, no ionizing radiation, quick evaluation at bed side and no patient preparation required. Ultrasound is also a great tool in follow up of vascular lesions in the neck as many of them are treated with local steroids. MRI is another great tool due to its multiplanar capability and to assess the deeper extent of the lesions however it is time consuming and requires sedation in pediatric age group, hence ultrasound a preferred modality.
Citation: Rajesh C Kamble., et al. “Utility of Ultrasound and Colour Doppler in Evaluation of Pediatric Vascular Lesions in the Neck".Acta Scientific Otolaryngology 3.4 (2020): 37-45.
Copyright: © 2021 Rajesh C Kamble., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
