Vishal Soni1*andMegha Sanghvi2
1Laparoscopic Gastro-Intestinal Surgeon, Department of Surgical Gastroenterology, Zydus Hospital, Ahmedabad, Gujarat, India
2Consultant Radiologist, Zydus Hospital, Ahmedabad, Gujarat, India
*Corresponding Author: Vishal Soni,Laparoscopic Gastro-Intestinal Surgeon, Department of Surgical Gastroenterology, Zydus Hospital, Ahmedabad, Gujarat, India.
Received: March 19, 2021; Published: April 12, 2021;
div class="tab">A 26-year-old Army man with a pre-operative clinical diagnosis of Pilonidal Disease was found to have a long lateral track extension intra-operatively. Surgery was abandoned and the patient was subjected to further radiological, microbiologicaland histopathological tests for etiology. After extensive work up, he was subjected to surgery with an excision of about 25 cm track and primary closure of the wound. He made uneventful recovery with excellent wound healing. Final histopathology report showed it to be Non-granulomatous Inflammation, without any hair elements due to which we would like to term it as a case of Idiopathic Natal Sinus (INS) and not a Pilonidal Disease. 4 year follow up has shown no recurrence.
Keywords: Sinus; Pilonidal; Natal Cleft Abscess; Atypical Sinus; Idiopathic Natal Sinus
A 26 yr old male Army personnel presents with 6 months history of wound 3 cm above natal cleft with purulent discharge with no significant past history. No other medical conditions were found. He was treated with multiple antibiotics and dressings without relief. Clinical examination, Blood investigations, Local part USG and X-rays were doneand a working diagnosis of Pilonidal Disease was made. The patient was taken for Excision with Local Flap Closure. Intra-operative instillation of diluted Hydrogen Peroxide and probing revealed a long lateral extension of the cavity almost reaching the left greater trochanter with no other lesions or signs of inflammation on the skin (Image 1). Further surgery was abandoned in view of uncertain diagnosis and to rule out a possible granulomatous disease. Pus and Track wall tissue were collected for analysis.

Figure 1:Opening in the upper part of natal cleft.
MRI was done, it revealed a single subcutaneous and partly intra-muscular track (in the Gluteal region) extending from the wound above the natal cleft to Left Greater Trochanter region. No involvement of bone, joint and deeper tissue was found (Image 2). Tissue Culture/Sensitivity grew Methicillin Sensitive Staphylococcus Aureus. ZeilNeelson Stain, Gene Xpert was negative, special stains for fungal elements were negative. He was treated with appropriate antibiotics for 10 days.
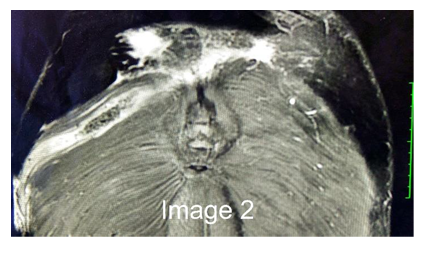
Figure 2:MRI delineation of the sinus tract.
The TB culture was negative at 6 weeks following which the patient was planned for surgical excision. There were no signs of wound healing. Intra-Op the external opening was cannulated with an 8 Fr. Infant feeding tube, Methylene blue - Hydrogen peroxide instillation was done, sinus was probed and track delineated. An innovative coring technique was planned for track excision by placing multiple (three) small incisions about 5cm long and 5 cm apart along the length of the track. A total of 25 cm long track was cored out (Image 3). The track showed thick wall with granulation tissue without any hair content and a cavitatory expansion on both ends. A soft suction drain was placed in the subcutaneous plane and wounds closed in layers with Vicryl 3-0 and Ethilon 2-0 (Image 4).

Figure 3:Multiple small incisions placed along the tract.
Figure 3:Single long intact tract with expansion at both ends.
Final histopathology report revealed a chronic non-granulomatous inflammation, Tuberculosis was conclusively ruled out. Drain was removed on POD3. The wound healed completely by post-operative day 10 (Image 5) and suture removal was done.

Figure 5:Wound at post-operative day 10.
Patient was followed up at 1month, 2 month and 3 months after definitive surgery with no recurrence or wound related issue (Image 6). The patient has been now followed up for 4 years without any recurrence or symptoms.

Figure 6:Wound at post operative day 90.
To call it a Pilonidal Disease was a question due to absolute absence of hair elements[1]. Atypical PNS (Pilonidal Natal Sinu) have been reported, however hair elements and foreign body reaction has been central to the pathogenesis[2]. Presence of an isolated lateral track with no midline cavity/pits/sinuses hasn’t been mentioned with respect to Pilonidal Sinus Disease. In our case the clinical examination didn’t reveal any hair element from the content in the sinus or in the track wall and even in the final histopathological report. Regarding the possible etiology, due to presence of an intra-muscular component, a possibility of post blunt traumatic sequelae from an organized hematoma could exist. In our case, we did suspect Tuberculosis/granulomatous disease, as reported in few case reports [3]. However, it was conclusively ruled out by negative Radiological, Microbiological and Pathological tests. Thus, in absence of any identifiable etiology, we propose to term it as Idiopathic Natal Sinus (INS).
The lateral extension wasn’t detected on pre-operative ultrasound, possibly due to the intra muscular course and low suspicion of such a finding. Usage of MRI in evaluation of any such discharging sinus is of paramount importance and should be used non-hesitantly[4]. The initial clinical diagnosis became questionable due to intra-operative findings, thus the importance of thorough examination under anaesthesia at the start of the surgery and alteration of plan, if any atypical or unexplained findings are encountered. Abandoning a planned surgery for an elective case was deemed appropriate in setting of surprise findings intra-operatively and we strongly recommend this practice.
A long incision was thought to be morbid for healing and thus as a modification was made to conventional long incision in form of multiple interrupted short incisions along the track - coring technique was used. It successfully translated into an uneventful, completeand quick wound healing. The patient had to be subjected to 2 surgeries but made an uneventful recovery.
None.
VS was involved in initial patient assessment, decision making and surgical care. MS contributed in radiological diagnosis, writing of the manuscript and follow-up of patient. Both the authors read and approved the final manuscript. Ethics approval and consent to participate Ethics was not required for this study as it is a case report of a onetime clinical event.
Written permission for publication of this report and the individual clinical data was obtained from the patient and is available for review by the editor.
The authors declare they have no competing interests.
Citation: Vishal Soni and Megha Sanghvi. “All Sinus in Natal, Always Pilonidal?". Acta Scientific Gastrointestinal Disorders 4.5 (2021):19-21 .
Copyright: © 2021 Vishal Soni and Megha Sanghvi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
