Abhishek M Bhagat*, Geeta Bhuvanagiri and Pallavi Bhyri
Department of Dentistry, Manipal College of Dental Sciences, Manipal, India
*Corresponding Author: Abhishek M Bhagat, Department of Dentistry, Manipal College of Dental Sciences, Manipal, India.
Received: July 18, 2024; Published: August 26, 2024
Citation: Abhishek M Bhagat. “Do The Alcoholic Beverages Affect Bonding of Glass Ionomer Cement to Dentin??". Acta Scientific Dental Sciences 8.9 (2024):61-66.
Introduction: Glass ionomer cement was introduced as restorative material, consisting of alumino-fluorosilicate glass powder and polyacrylic acid in aqueous form. With the initiation of an acid base reaction, forming a gel substitute [1,2]. Many studies suggest various qualities of Glass ionomer cement that can aid the affected dentin remineralization process. This study is to test the effect of alcoholic beverages on the shear bond strength of Glass ionomer cements to dentin.
Aim: The aim of this study is to test the effect of alcoholic beverages on the shear bond strength of GIC to dentin.
Materials and methods: A total of 140 extracted mandibular molars were mounted into acrylic blocks and trimmed to expose the dentin. The samples made were divided into 2 groups (70 each) and restored with either Type IX GIC or Type II GIC, condensed onto the sample in a cylindrical shape of 5mm diameter. These samples were tested after getting dipped in different types of alcoholic beverages for 30 days.
Result: The highest reduction in bond strength was seen in samples of group 2b (type II 0.95 ± 0.15 type IX 0.93 ± 0.45) followed by group 2a (type II 1.11 ± 0.27, type IX 3.70 ± 0.93), group 4b (type II 1.30 ± 0.21, type IX2.55 ± 0.36), and group 4a (type II 4.77 ± 0.091, type IX 4.69 ± 0.47). Maximum shear bond strength was seen in Group 1(type II 5.81 ± 0.23, type IX 7.35 ± 0.84).
Conclusion: The study concludes that the shear bond strength of glass ionomer cement to dentin reduces with the consumption of alcoholic beverages having low pH and higher frequency of intake.
Keywords: Alcoholic Beverages; Composite Resin; Shear Bond Strength; Cough Syrup; Gin; Rum
Glass ionomer cements were discovered by Alan Wilson and Brian Kent at the Laboratory of the Government Chemist, London, in the late 1960s. They were introduced as restorative dental material in 1972 and have a history of long and extensive use. These materials consist of an alumino fluorosilicate glass powder and an aqueous polyacrylic acid and the cement formation arises from the acid-base reaction between components [1,2].
Glass Ionomer Cements are used in restorative dentistry for a variety of qualities such as chemical adhesion to enamel and dentin, less volumetric contraction, preservation of the pulp, coefficient of thermal expansion like dentin, low solubility in the oral environment and release of fluoride, that can aid the affected dentin remineralization process [3]. Some of their less desirable characteristics are sensitivity to moisture, low mechanical strength, and low wear resistance [4].
Due to the above-mentioned properties glass ionomer cements find unique uses in pediatric dentistry, atraumatic restorative treatment, restoration of cervical abrasions and Class V cavity preparations [5]. Its anti-cariogenic property is also useful when treating geriatric patients [6]. In uncooperative patients i.e. younger patients or especially abled patients, where extensive cavity preparation, moisture control with rubber dams or all the steps of adhesion for composites cannot be performed, GICs can be used as an effective replacement [7]. GICs are the materials used for tooth repair by the ART technique. The technique has been developed with the aim of preserving dental structure and to provide preventive and curative care in low- and middle-income countries [8]. ART follows the concept of minimal intervention and involves hand excavation of carious tissue in lieu of rotary instruments [9]. The use of high viscosity conventional GICs i.e. Type IX GIC has been recommended for ART due to their improved mechanical properties, which are related to the size and type of filler particle content [10,11]. For these reasons, Type II and Type IX GICs have been selected for this study.
While the properties of these materials have been extensively studied, the long-term clinical performance is dependent on various factors including the effect various foods and drinks have on the material. Due to low pH and ethanol content, alcoholic beverages can produce erosion and modify the properties of various restorative materials [12,13]. They can also influence the restoration- tooth interface, thereby affecting the longevity of the restoration in the oral cavity [14]. To evaluate this effect, two alcoholic beverages with varying alcohol concentration have been chosen. Given that GIC is extensively used in pediatric dentistry and with flu being a very common childhood disease, another parameter ‘Cough Syrup’ has been introduced.
Various studies have been conducted to understand the effect of alcohol on surface roughness and microhardness of GIC [15], to the best of our knowledge there are no studies done to evaluate the effect of alcoholic beverages on the shear bond strength of GICs. Hence, this study tested the hypothesis that alcoholic beverages affect the shear bond strength of GIC to dentin.
140 intact mandibular molars extracted in the Department of Oral and Maxillofacial Surgery and other clinics in and around Manipal were collected. The collected samples were then dipped into 6% hydrogen peroxide to remove any soft tissue debris. After cleaning and disinfection with betadine solution, the teeth were mounted into acrylic blocks and trimmed to expose the dentin.
These samples were divided into 2 groups (70 each) to be restored with either Type IX GIC or Type II GIC. The materials were mixed according to the manufacturer's instructions with a powder to liquid ratio of 2.7: 1 for Type II GIC (lot no: 1906151) and 3.6:1 for Type IX GIC (lot no: 2101051 [liquid]). The mixed cement was then condensed onto the sample in a cylindrical shape of 5mm diameter.
The samples from each of these groups were further divided randomly into 4 groups. Control (Group 1), Cough Syrup (Group 2), Gin (Group 3), Rum (Group 4). Groups 2, 3 and 4 were again divided into Moderate (Groups 2a, 3a, 4a) and Heavy (Groups 2b, 3b, 4b) consumption groups. The samples were soaked in their respective test solutions for 90 mins daily for groups 2a, 3a and 4a and 30 mins every alternate[A[M1] day for groups 2b, 3b and 4b according to USD guidelines. Between the soaking periods samples were incubated in artificial saliva. This process was done for 30 days after which the samples were tested for the shear bond strength using Instron 3366 UTM.
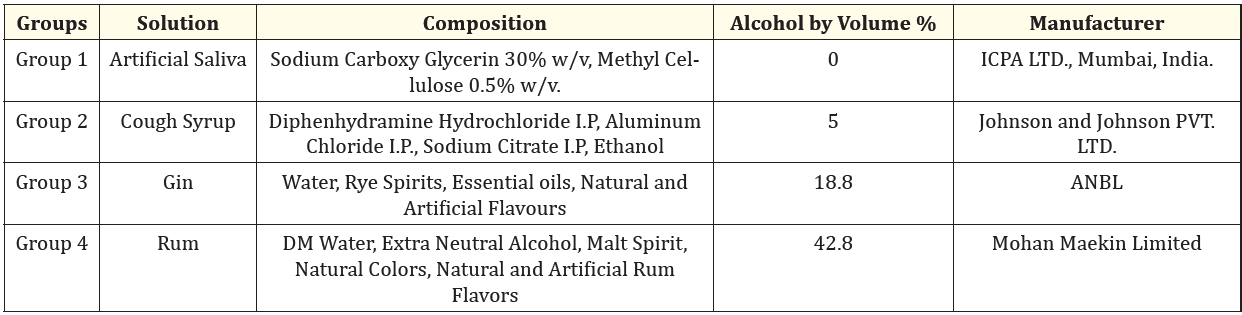
Table 1
Shear bond strength was calculated according to the following formula and expressed in MPa.
Stress = Failure load (N)/surface area (mm2)
Table 2
The shear bond strength of all the groups is presented in table 2. The highest reduction in bond strength was seen in samples of group 2b followed by group 2a, group 4b, and group 4a. Maximum shear bond strength was seen in Group 1.

Figure 1: Molar with exposed dentin mounted onto an acrylic block.

Figure 2: Prepared sample with GIC type II condensed in a cylindrical shape of 5mm diameter.

Figure 3: Glass Ionomer Cement Type II.

Figure 4: Glass Ionomer Cement Type IX.
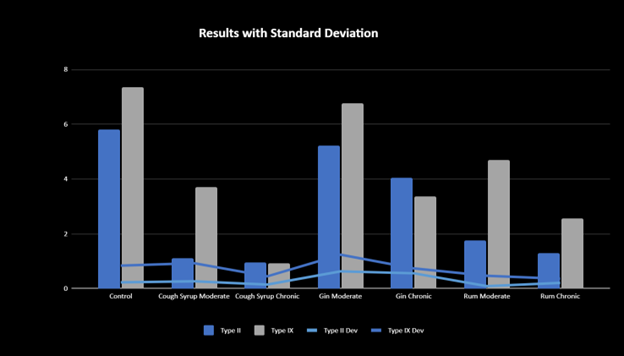
Figure 5: Results acquired after shear bond strength testing using Instron 3366 UTM. X Axis: testing solution. Y Axis: Shear Bond Strength in MPa. Blue bars of the chart mark the shear bond strengths of Glass Ionomer Cement Type II whereas the gray bars mark the shear bond strengths of GIC Type IX. Standard Deviation is expressed via the line graph.
Although GIC has been in market as a restorative material for 5 decades, it has gained popularity with its recent advances and its increased use in ART, Pediatric and Geriatric Dentistry [16]. GIC and its various properties have been extensively studied and enormous improvements have been made to increase its retention and longevity in the oral cavity. Despite these, the shallow hybrid layer at the tooth restoration interface remains the Achilles heel of a glass ionomer restoration [17]. The clinical success of a restorative material depends on good adhesion with the dentinal surface to resist the dislodging forces. Though compressive and tensile strengths are important parameters to be evaluated, in the present study, we have evaluated shear bond strength as it assumes much importance to the restorative material clinically because major dislodging forces at the tooth restoration interface have shearing effect. Therefore, higher shear bond strength implies better bonding of the material to tooth [18].
The strength of the bond to hard tissues of the teeth is dependent on several factors. These include the heterogeneity of tooth structure and composition, the features of the dental surface exposed after cavity preparation, and the characteristics of the adhesive itself [17,19]. Apart from all these, adhesive restorations in the oral environment are constantly subjected to various interactions between food and drinks consumed, which have different pH and solubility levels. Inevitably, the varying pH can cause changes in the mechanical and chemical properties of the cement.
Glass Ionomer Cements were used in this study as they are ideal for uncooperative patients. The property of chemical adhesion to enamel and dentin exhibited by GICs make them ideal uncooperative, pediatric, and geriatric patients. It is also the material of choice when extensive cavity preparation is not achievable. Other properties such as preservation of the pulp, coefficient of thermal expansion like dentin, low solubility in the oral environment and release of fluoride, that can aid the affected dentin remineralization process distinguish GIC from other adhesive resins [3].
Alcoholic drinks have been consumed since ancient times which play an important social role in many cultures. These beverages are available as three main classes: beer, wine, and spirit, with our choice of alcoholic beverage being rum and gin. Rum and gin are forms of spirits, that are produced by distillation [20,21]. in the 21st century the consumption of gin and rum has increased due to the spirit movement which has led to the reduction in the distillation prices thereby reducing the overall MRP [22,23]. These spirits are widely consumed by the adult population of drinking age.
One form in which the pediatric population consumes alcohol is through cough syrups [24]. Cough syrups are available in both medicated and OTC form and are used as a deterrent to childhood cough, rhinitis and congestion [25]. Alcohol is a major component of most cough syrup and acts as a cosolvent to increase drug solubility, a preservative due to its antimicrobial activity and sedative [26,27]. According to FDA guidance, the alcohol concentration limit of oral OTC medication is 10% for adults and children above 12 years, 5% for children aged 6-12, and 0.5% for children under 6 years [28].
The present study was performed to determine the effect of these three forms of alcohol consumption, i.e. rum, gin and cough syrup on shear bond strength of GIC to dentin. The effect of exposure to alcohol by moderate and heavy consumers was also taken into consideration separately. Artificial saliva was used as control to imitate the oral cavity environment.
The United States Dietary Guidelines define moderate alcohol drinking for women as up to 1 drink/day and for men up to 2 drinks/day, while heavy drinking is defined as consuming eight or more drinks/week for women and 15 or more drinks/week for men [29]. The peak level of blood alcohol is achieved in 30–90 min after consumption of alcoholic beverage [30]. Hence, a soaking time of 30 min every alternate day for moderate consumption group and 90 min daily for heavy consumption group was chosen.
Based on 30 days' experimental period, all the groups showed significantly decreased bond strength irrespective of their exposure when compared with the control. The highest reduction in shear bond strength was obtained with Group 2, followed by Group 4 and then Group 3. Therefore, the hypothesis was confirmed since the alcoholic beverages reduced the shear bond strength of GIC to dentin at the end of the experimental period. Increased reduction in shear bond strength despite low ABV in cough syrup can be attributed to other chemical compounds present in it. Further research into these compounds is essential to determine which compound has the most detrimental effect.
Within the limitations of the study, it can be concluded that the shear bond strength of glass ionomer cement to dentin reduces with the consumption of alcoholic beverages having low pH and higher frequency of intake [A[M4]. However, various other factors affect shear bond strengths of cements including compounds present in various foods, beverages and medicines, physical parameters while mixing and setting of the cement in the oral cavity, chronic diseases that affect the oral environment including conditions that cause xerostomia etc. All of these must be considered before a conclusive comment can be made regarding the shear bond strength in the oral cavity.
Copyright: © 2024 Abhishek M Bhagat. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff








ff
© 2024 Acta Scientific, All rights reserved.