Marcelo Salmazo Castro1, Ana Virginia Santana Sampaio Castilho1, Lucas José de Azevedo-Silva2, Lorrayne Farias dos Santos3, Eliel Soares Orenha1 and Silvia Helena de Carvalho Sales-Peres1*
1Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru School of Dentistry, University of São Paulo, Brazil
2Department of Prosthodontics and Periodontology, Bauru School of Dentistry, University of São Paulo, Brazil
3Bauru School of Dentistry, University of São Paulo, Brazil
*Corresponding Author: Silvia Helena de Carvalho Sales Peres, Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru School of Dentistry, University of São Paulo, Brazil.
Received: March 15, 2021; Published: April 08, 2021
This systematic review aimed to investigate the COVID-19 biological risk based in knowledge, attitudes and perception of dentists during COVID-19 pandemic and to establish a clinical protocol based on the literature. The protocol was conducted in accordance to PRISMA Statement and registered on International Prospective Register of Systematic Reviews (CRD42020200258). PubMed, Embase and SciELO were systematically searched, using the key terms “coronavirus infections” AND “dentists”. Four articles were selected for qualitative and ten for quantitative analysis. The overall studies reported characteristics of dentists (n = 12,913) who completed survey questionnaires: male (n = 6,690; 51.8%); knowledge: transmission route (n = 1,892; 14.65%), use of personal protective equipment (PPE) (n = 2,418; 18.7%) and signs and symptoms (n = 1,489; 11.5%); attitudes: urgency treatment (n = 2,633; 20.4%), handwashing (n = 5,548; 43%), reducing patients in waiting room (n = 3,020; 23.4%), and use of masks (n = 4,068; 31.5%); and perception: infection risk (n = 2,387; 18.5%). The clinical protocol includes procedures before appointments, correct handling of the operative area, and use of correct PPE. The primary COVID-19 biological risks are infectivity and horizontal transmission. The clinical care protocol in dentistry should be adopted by all dentists to reduce biological risk. Thus, dentists may play an important role in the prevention and interruption of SARS-CoV-2 transmission chain.
Keywords: Coronavirus Infections; Containment of Biohazards; Dentists; Dentistry; Clinical Protocol
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the causative agent of coronavirus disease 2019 (COVID-19), an infectious disease characterized by several important systemic disorders, such as pneumonia associated with coronavirus. The main symptoms of the disease are categorized into mild (fever, cough, myalgia, fatigue and sputum) and severe (cyanosis, tachypnea, chest pain, hypoxemia, dyspnea, and require clinical assessment) [1-3]. Most patients have mild symptoms, and in more severe cases, they can progress to pneumonia [4].
Among healthcare professionals, dental surgeons have been highly exposed to SARS-CoV-2 infection [5-7]. These professionals routinely perform procedures using instruments that generate aerosols (small particles), which can be inhaled within the work environment, exposing both the clinician and the patient to infection. Dental professionals must protect the patients from the spread of all infectious diseases by adopting safe practices in the performance of their work and making dental procedures safe [8].
According to a scientific report published by the World Health Organization, the SARS-CoV-2 can be transmitted through respiratory droplets from direct contact with an infected person (distance less than 1 m), indirect contact with contaminated surfaces or objects and aerosol produced during procedures performed on infected patients [9]. Hence, dental and health organizations have published recommendations to postpone all elective dental treatments and non-essential procedures and limit services to urgent and emergency visits only.
Dental health personnel (DHP) should be aware of the transmission mechanisms and infection control procedures, be able to identify patients with signs and symptoms of COVID-19 and have a clear understanding of the characteristics of a dental emergency, an urgent dental care and a non-emergency dental treatment [10].
There is 100% chance of acquiring the infection when an individual comes in contact with a COVID-19 patients’ saliva; saliva samples can also grow the live virus. Hence, the potential infectivity of saliva must be strongly considered [11]. Thus, dental offices, both in the public and private sectors, are considered as high-risk environments for cross-infection among patients, dentists, and healthcare professionals in the clinical setting. Elective dental treatments and non-essential procedures must be postponed and only emergency care must be provided. Dentists should consider that a substantial number of individuals who do not show signs and symptoms of COVID-19 may be infected and spread the virus [10].
Therefore, preventive strategies must be improved, especially for dentists, to reduce the risk of acquiring COVID-19 [12]. Currently, one of the main challenges in dental care is the difficulty in identifying infected patients, due to the need for an adequate diagnostic pattern and the possibility of exposure to an asymptomatic patient. Hence, every patient should be considered as an infected individual to the risk of infection. Therefore, this systematic review aimed to investigate the COVID-19 biological risk supported by the level of knowledge, attitudes and perception of dentists during the COVID-19 pandemic. We also propose to create a new clinical care protocol based on the gaps found in the recent literature.
The data in this systematic review were reported according to the National Health Service Centre for Reviews and Dissemination [13] and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA Statement) guidelines [14] based on Cochrane collaboration (www.cochrane.org). The complete work protocol was registered in the International Prospective Register of Systematic Reviews (CRD42020200258). The eligibility criteria were defined in relation to the participants, interventions, comparisons, outcomes, and study design as recommended by the PRISMA Statement. In this systematic review, the following questions were raised: 1) What has been changed in dentistry practice during the COVID-19 pandemic? 2) What level of knowledge does the dentists have regarding the disease? 3) Are the dentists using the correct preventive measures against the spread of coronavirus? 4) What new protocols can be adopted for dental care?
Search strategy and selection criteriaPubMed, Embase, and SciELO were systematically searched, using the following key Medical Subject Headings terms: “coronavirus infections” AND “dentists”. Furthermore, the reference list was reviewed to identify other potentially relevant studies. The last search was conducted on June 26, 2020.
As the eligibility criteria, we selected studies in English published in peer-reviewed journals that have addressed the questions in surveys using epidemiological data, reported the protective measures, and discussed the knowledge and the prevention and control practices of dentists during the COVID-19 pandemic. Articles with protocols for managing COVID-19 were also considered. Duplicate publications and articles that did not achieve the objectives of this systematic review were excluded. Similarly, publications without a research protocol such as opinion article, correspondence, editorials and letters were also excluded. Figure 1 shows the procedure of the literature search.
Data extractionThree investigators participated in each phase of the review and independently screened the titles and abstracts of the articles obtained during the search based on the inclusion criteria. The investigators screened the full text reports and determined if they met the inclusion criteria. Discrepancies between the reviewers were resolved by discussion and consensus, and the final results were reviewed by the senior investigator. The following data were extracted from the included articles: study design, methodology, year of data collection, sample size and characteristics, outcomes, exposure, and comparators.
Quality appraisal and risk of biasThe cross-sectional studies were appraised using appropriate tools for each study design. The Newcastle-Ottawa Scale (NOS) and NOS-derived survey scale [15] were used to assess the risk of bias (ROB) in three domains, and the maximum score is 9 points: 1) selection of study groups (0 - 4 points), 2) comparability of groups (0 - 2 points), and 3) ascertainment of exposure and outcomes (0 - 3 points) for cross-sectional studies [14]. Scoring was undertaken by two reviewers, with a third reviewer resolving any disagreements. Studies were considered at low ROB when the overall scores were 9 - 10, moderate when scores were 6 - 8, and high when the scores were 0 - 5. Research questions were developed based on the NOS questions covering all three domains so that the authors could provide detailed information about their studies.
Summary measuresQuantitative data were grouped based on the following relevant variables: degree of qualification, occupation area, and years of practice. Data on knowledge, practices and attitudes of healthcare professionals as well as their perception of the new way of working in the clinical setting were also categorized. With regard to the protocol studies, the main points in each study were selected, grouped according to similarity, and presented in a table. The data were analyzed and grouped by all three researchers, and the tabulation of all data was performed by one researcher. After tabulating the data, the data were reviewed by another researcher, hence decreasing the possibility of disagreements.
Figure 1 shows a flowchart illustrating the selection of studies for inclusion in the systematic review. After searching all scientific databases for related studies, a total of 87 articles were selected; after removing the unrelated and duplicate articles, 19 were assessed for eligibility. Finally, only 14 articles were included in the qualitative analysis, while 9 were included in the quantitative analysis.

Figure 1: PRISMA 2009 flow diagram.
Studies characteristicsNine articles fulfilled the criteria for quantitative and qualitative evaluation and were included in the final step of the systematic review. The final articles were cross-sectional studies and assessed the knowledge, attitudes and practices, as well as the perception of dentists regarding the COVID-19. These studies underwent quality assessment using NOS and obtained a score ranging from 7 to 8; this score indicated that the studies had moderate quality. The other four studies reported the clinical care protocols. These protocols were used for a brief qualitative review and as a basis for establishing a new clinical protocol.
Subgroup and overall summary of sample in the systematic reviewA detailed description of the included studies is shown in table 1. The pooled data from studies (n = 12,913) included the characteristics of dentists who completed the survey questionnaire: associations of male gender (n = 6,690; 51.8%); qualifications: postgraduate (n = 4,680; 36.2%), graduate (n = 4,214; 32.6%), auxiliary staff (n = 202; 1.56%), and interns (n = 162; 1.2%); occupational area: academic (n = 888; 6.9%), clinician (n = 10,931; 84.5%), and others (n = 486; 3.8%); years of practice (n = 6,206): 0–10 years (n = 2,997; 48.3%), > 10 years (n = 3,105; 50.0%), and currently not practicing (n = 103; 1.7%).
|
Studies |
Kamate., et al. 2020 |
Stefani., et al. 2020 |
Khader., et al. 2020 |
Consolo., et al. 2020 |
Moraes., et al. 2020 |
Cagetti., et al. 2020 |
Quadri., et al. 2020 |
Ahmed., et al. 2020 |
Duruk., et al. 2020 |
Total |
|
Location |
Worldwide |
Italy |
Jordan |
Italy |
Brazil |
Italy |
Saudi Arabia |
Worldwide |
Turkey |
|
|
Quality of studies (NOS) |
7 |
8 |
8 |
8 |
8 |
7 |
8 |
7 |
7 |
|
|
Sample |
860 |
1500 |
368 |
356 |
3122 |
3599 |
500 |
650 |
1958 |
12.913 |
|
Gender |
|
|
|
|
|
|
- |
|
|
|
|
Male |
- |
664 |
245 |
215 |
2326 |
2493 |
|
160 |
587 |
6.690 (51.8) |
|
Female |
- |
836 |
123 |
141 |
790 |
1106 |
|
490 |
1371 |
4.857 (37.6) |
|
Age (median) |
- |
- |
32.9 |
|
38 |
- |
- |
- |
32.5 |
- |
|
Qualification n (%) |
|
|
|
- |
|
- |
|
|
|
|
|
Post-graduate |
301 (36.5) |
945 (63.0) |
112 (30.4) |
|
2363 (75.7) |
|
136 |
139 (22.0) |
684 (34.9) |
4.680 (36.2) |
|
Graduate |
545 (63.5) |
870 (58.0) |
256 (69.6) |
|
758 (24.3) |
|
- |
511 (78.0) |
1274 (65.1) |
4.214 (32.6) |
|
Auxiliar staff |
- |
- |
- |
|
- |
|
202 |
- |
- |
202 (1.56) |
|
Interns |
- |
- |
- |
|
- |
|
162 |
- |
- |
162 (1.2) |
|
Practing n (%) |
|
|
|
|
|
|
- |
|
|
|
|
Academic |
202 (23.5) |
53 (3.5) |
112 (30.4) |
- |
- |
- |
|
- |
521 (26.6 |
888 (6.9) |
|
Private |
559 (65.0) |
1,447 (96.5) |
228 (62.0) |
356 (100) |
2,692 (86.2) |
3599 (100) |
|
613 (94.3) |
1437 (73.4) |
10.931 (84.5) |
|
Other |
99 (11.5) |
- |
28 (7.6) |
- |
359 (13.8) |
- |
|
- |
- |
486 (3.8) |
|
Years of practice n (%) |
|
|
|
|
|
- |
- |
- |
- |
6.206 (100) |
|
0 - 10 |
712 (81.7) |
465 (31.0) |
244 (66.3) |
80 (22.5) |
1,496 (47.9) |
|
|
|
|
2.997 (48.29) |
|
> 10 |
45 (5.3) |
1,035 (69.0) |
124 (33.7) |
226 (77.5) |
1,625 (52.1) |
|
|
|
|
3.055 (49.22) |
|
Currently not practicing |
103 (12.0) |
- |
- |
- |
- |
|
|
|
|
103 (1.66) |
Table 1: Socio-demographic distribution of the respondents.
Knowledge, attitudes/practices, and perception/psychological aspects during the COVID-19 pandemicData regarding the dental professionals’ knowledge, attitudes, and practices, as well as perception and psychological aspects during the COVID-19 pandemic are shown in table 2.
|
Studies |
Evaluation |
Knowledge |
Attitudes and practices |
Perception and psychological aspects |
|
Kamate., et al. 2020 |
Knowledge, attitudes and Practices regarding COVID-19 |
Heard about COVID-19 = 855 (99.4) Affected system = 736 (85.6) Transmission routes = 839 (97.6) Signs and symptoms = 850 (98.8) Vaccine availability = 586 (68.1) Mode of spreading = 829 (96.4) Protection from masks = 858 (99.8) Method of diagnosing = 552 (64.2) Fatality = 825 (95.9) |
Possible to spread awareness to other dentists = 860 (100) Effectiveness of hand hygiene and PPE in preventing infection = 860 (100) |
|
|
Stefani., et al. 2020 |
Knowledge about transmission, symptoms and attitude in treating potentially COVID-19 infected patients |
Appropriate PPE = 887 (59.1) Correct symptoms = 198 (13.2) Transmission routes = 1,053 (70,2) Correct information about Vaccine availability = 1,493 (99.5) |
Not involved in covid-19 patients’ treatment = 1,028 (68.5) Urgency Treatment only = 123 (8.2) |
Not trained sufficiently = 858 (57.2) |
|
Khader., et al. 2020 |
Level of awareness, perception and attitudes and infection control regarding the COVID-19 |
Correct incubation period = 162 (44.0) Infected patients may not present symptoms = 127 (34.5)
|
Frequently clean hands = 354 (96.2) Frequently clean and disinfect surfaces = 347 (94.3) Correct PPE use = 342 (92.9) All staff members with PPE = 304 (82.6) Place suspect/known infected patient in ventilated room = 284 (77.2) |
COVID-19 dangerous = 65 (17.7) Important to educate people to prevent the spread of the disease = 360 (97.8)
|
|
Consolo., et al. 2020 |
Dentist behavior and analysis of reactions in relation to Sars-CoV-2 pandemic restrictive measures |
Not working/emergency only = 356 (100) Increase/modify PPE use = (77) Information of PPE use to staff = 279 (78.4) Phone triage = 341 (95.8) |
Negative impact on their professional activity = 265 (74.4) Experience fear intensely = 15 (4.2) Experience anxiety intensely = 22 (6.2) Experience concern intensely = 57 (16) Felt intensely sad = 49 (12.6) Experienced intense anger = 33 (9.3) |
|
|
Moraes., et al. 2020 |
Impact of the pandemic on behavior of dental practice routines |
Lower patient volume = 994 (32.5) Emergency only = 1,325 (43.4) Not working due to pandemic = 546 (17.9) Online training or general instructions = 2,406 (77.6) Practical training = 134 (4.3) |
None training for specific measure = 559 (18.0) Very high impact = 1,617 (53.1) Increased costs: Yes, but prices were not adjusted = 1,432 (64.9) Yes, and prices were adjusted for patients = 328 (14.9) |
|
|
Cagetti., et al. 2020 |
Knowledge about symptoms/signs, protective measures, awareness, and perception levels regarding COVID-19 among |
Enough knowledge on the disease and protective measures = 2,537 (70.49)
|
Phone Triage = 2542 (82.37 Spaced appointments = 2656 (86.07) Deferring therapies in risk groups = 1912 (61.96) Taking co-workers’ body temperature = 656 (21.26) Taking Patient’s body Temperature = 725 (23.49) Disinfection of operative devices = 2525 (81.82) Verify the patient’s health status = 2568 (83.21) Washing the patient’s hands = 2413 (78.19) Space of at least one meter between patients = 2312 (74.92) Mask for the patient = 1011 (32.76) Frequent ventilation of waiting rooms = 2746 (88.98) Ventilation of the operating area for at least 10 min after each patient = 2379 (77.09) Removal of magazines and books from the waiting area = 2418 (78.35) Storage of coats, bags, and other items outside the operating area = 2103 (68.15) Pre-operative rinse with mouthwash = 3,110 (86.4) Disinfection of surfaces with usual disinfectant with other active ingredients = 1875 (60.76) Washing hands before and after procedures = 2828 (91.64) Removal of all disposable protective devices and disinfection of devices = 2484 (80.49) |
Profession at risk = 2,321 (64.50) Confident in avoiding the infection = 77 (2.13) Risk of transmission during dental practice is higher than in a supermarket = 2,465 (68.50) |
|
Quadri., et al. 2020 |
Knowledge on COVID-19 among the Dental care health workers |
COVID-19 correct system disorder = 173 (34.6) Sneezing as a symptom = 427 (85.4) Correct safe distance = 269 (53.8) Low risk group = 266 (53.2) Risk for patient and HCW = 305 (61.0) Air borne = 250 (50.0) High morbidity group = 463 (92.6) Correct incubation period = 350 (70.0) Correct first symptoms = 441 (88.2) Common symptoms flu and COVID-19 = 50 (10.0) Antibiotic for treatment = 41 (8.2) Vaccine availability = 29 (5.8) |
||
|
Ahmed., et al. 2020 |
Dentists’ anxiety and fear and knowledge about various practice modifications to combat COVID-19 |
Aware of the Mode of Transmission of COVID-19 = 631 (97.0) Updated with CDC or WHO Guidelines for cross-Infection Control = 588 (90.0) Surgical Mask is enough = 72 (11.0) N-90 Mask should be Routinely Worn in Dental Practice = 548 (84.0) Aware of authority to contact if come across a suspected patient = 519 (80.0) |
Asking patient’s travel history before Treatment = 532 (82.0) Taking Patient’s Body Temperature = 530 (81.0) Deferring Treatment in symptomatic patients = 512 (78.0) Routinely Follow universal Precautions of Infection Control = 583 (89.0) Use of rubber dam = 93 (14.0) High-Volume Suction in Practice for Every Patient = 499 (76.0) Ask patients to rinse their mouth before treatment = 160 (24.0) Wash hands with soap and water/use sanitizer before and after treatment = 611 (94.0) |
Afraid of getting infected from a Patient/Co-Worker = 556 (87.0) Anxious when Providing Treatment to a Patient Coughing or Suspected = 585 (90.0) Close Dental Practice until the cases decreases = 431 (66.0) Feel Nervous talking in close with Patients = 467 (72.0) Afraid of taking infection from dental office to family = 600 (92.0) Afraid of getting quarantined = 505 (77.0) Anxious about the cost of treatment if Infected = 476 (73.0) Feel afraid because of COVID-19 deaths = 547 (85.0) |
|
Duruk., et al. 2020
|
Precautions taken by Turkish dentists in dental clinics during the COVID-19 pandemic
|
Sufficient own self-assessed Covid-19 knowledge = 942 (48.1)
|
Attended an informational meeting on Covid-19 = 522 (26.65) Use of mask = 1682 (85.9) Use of gloves = 1,891 (96.6) Use of goggles = 1,048 (53.52) Use of face shield = 1,377 (70.33) Frequent hand washing = 1,897 (96.88) Frequent hand sanitizing = 1624 (82.94) Ask patients about symptoms = 83 (4.24) Use of Rubber dam = 271 (13.84) Pre-operative rinse with mouthwash = 1,218 (61.21) Use of strong absorbent system during procedure = 1,249 (63.79) Decrease in aerosol generating procedures = 978 (49.95) Reduced the number of patient admission = 364 (18.6) Only emergency patients = 829 (42.3) Closed = 240 (12.3) |
Difficulty accessing protective equipment = 908 (46.37) Insufficient awareness among colleagues about COVID-19 = 647 (33.04) Low awareness among assistant HCW about COVID-19 = 615 (31.41) Low awareness among patients about COVID-19 = 1,716 (87.64) Concerned about being infected as a profession group at high risk = 1,358 (69.1) Worried about transmitting to your immediate environment = 1,886 (96.32)
|
Table 2: Knowledge, attitudes/practices and perception/psychological aspects data assessed in selected studies.
This study systematically reviewed several cross-sectional studies by conducting a questionnaire survey and using care protocols aimed at examining the strategies adopted by dental health professionals in providing patient care during the period of the COVID-19 pandemic. Considering the knowledge, attitude, and practices adopted by dental professionals during the COVID-19 pandemic, a protocol must be followed in order to prevent or interrupt the chain of COVID-19 transmission.
The dental team must take precautions to reduce the spread of infection. Adequate information and training must be provided these healthcare professionals to control infections in the dental office [16,17]. In Quadri., et al. [18], a questionnaire was administered to 706 dental health professionals. Of them, 500 were knowledgeable about COVID-19, while 206 were unaware of this disease. In the group that had no knowledge about COVID-19, after the training, a significant improvement (p < 0.05) was observed in the groups’ knowledge regarding the disease.
Dental care professionals should have sufficient knowledge regarding mode of COVID-19 transmission and other viral agents, the methods of identifying patients with active infections and measures that can protect them and their patients from acquiring COVID-19. The basic principle of infection control is to treat each patient as if they are infected and implement the correct protective strategies [19]. Previous studies have shown that even non-symptomatic patients can spread the virus [20,21].
Previous studies have evaluated the knowledge of dentists in relation to COVID-19 [18,22-25], signs and symptoms related to the disease [18,22-24,26], transmission routes [6,18,22,23], hygienic measures [6,8,10,27] and the importance of using PPE [6,8,10,18,22-25,27,28]. Health professionals must provide clear and easy guidelines for managing patients and must maintain a safe dental practice to reduce the risk of disease transmission [29].
Measuring the temperature of patients before dental treatment is an important step that should be adopted as a form of prevention in the care of infected patients. Some proposed methods have been adopted to measure temperature, such as less than a quarter of patients [24]. The dental assistant measures the body temperature without direct contact with the patient using infrared thermometers [6,8,26]; an initial telephone interview with the patient must be made in order to verify whether he or she had a fever or developed other signs of COVID-19 [24].
Two studies assessed the study patients for signs and symptoms of COVID-19 [17,24]. One study reported 474 dental surgeons with COVID-19 symptoms, 31 dental surgeons who tested positive for SARS-CoV-2, 16 individuals who developed the disease [24], 314 individuals with suspected COVID-19, and 33 individuals who tested positive for SARS-CoV-2 [17]. These data were used to verify whether testing of symptomatic professionals is an essential measure to prevent the spread of the disease. The primary method to prevent disease spread is to prohibit the symptomatic professionals from seeing their patients, mainly due to the large number of false-negative cases in relation to COVID-19 [30-32].
The spread of viral particles in the form of aerosols is considered as the primary route of COVID-19 transmission [2,33]. Dental surgeons should minimize the use of aerosol-generating procedures and the conscious implementation of this practice is recommended [6,26]. During dental procedures, inhalation of aerosols produced by instruments used in patients with COVID-19 increases the risk of disease spread. It is also possible to detect the presence of viral particles in the saliva of patients with COVID-19 [12], elective procedures should be postponed until the end of the acute phase and only urgent and emergency care should be provided [6,8,10].
Several studies have also been evaluated the attitude changes during the period of pandemic: anamnesis reported via telephone interview [8], decrease in the number of patients [17,24], care provided only during emergency cases [16,17,22,23], increased ventilation of the rooms after an appointment and local cleaning [8] and training of clinical staff on the correct use of PPE and other safety measures [16,17] were reported in the studies analyzed.
The use of PPE for the entire dental team is recommended, and the use of equipment that produces aerosols must be avoided [6]. If the use of these equipment is required during a dental procedure, absolute isolation must be implemented and high-power suction must be used in order to control and minimize the dispersion of contaminated aerosols. During radiographic examinations, extraoral measures must be preferred over intraoral ones, since the latter can stimulate greater salivary production, thus increasing the risk of contamination. There is currently no consensus on the correct use of solutions for mouthwash. Previous studies showed that dental surgeons are recommending various types of products without determining their effectiveness [24,25,28]. There is still insufficient scientific evidence to prove the effectiveness of a mouthwash against coronavirus, suggesting the need for further studies in this area.
The masks are used to protect professionals and patients, limiting the potential spread of infectious respiratory aerosols. They can be used with glasses to protect the mouth, nose and eyes, or with a face shield to provide more complete facial protection. The mouth, nose, and eyes serve as portals of entry of infectious pathogens [4]. Surgical masks are used to prevent large particles (such as droplets, sprays, or splashes) from reaching the nose and mouth [34]. Although masks are used to protect patients from healthcare professionals by minimizing exposure to saliva and other respiratory secretions, they do not create a seal on the skin of the face and are therefore not indicated to protect people from infectious diseases transmitted by air.
When treating patients with respiratory infections, particulate respirators such as N95 [4] should be worn by professionals [6,8,10,17,18,23,24]. In the study developed by Duruk., et al. [28], it was found that only 12% of professionals adhered to the use of an N95 mask. This low adherence led to an increase in the rate of contamination; hence, the dentists’ rate of adherence to this measure increased.
Disposable face shields may also be used in addition to protective glasses and masks. The facial protector covers other areas of the face besides the eyes. The face shields extend from the chin to the forehead, thus offering better protection of the face and eyes against splashes [35].
Cagetti., et al. demonstrated that half of the professionals included in their study used face shields. Meanwhile, Peditto., et al. suggested the adoption of glasses, protective visors and masks, even when performing procedures that do not generate aerosols [8].
Gloves are essential in all dental procedures. In most of the studies analyzed, professionals are knowledgeable and aware about the importance of using this item as an essential form of prevention [6,17,18,24]. Moreover, it is extremely important to maintain excellent hand hygiene practices before and after performing each procedure in order to protect all members of the dental team. Recent studies [8,17,18,23,24] reported a great number of professionals who adopted this measure as an essential prevention procedure.
Several studies have proposed a protocol to reduce the biological risk (Table 3). The studies analyzed provided an overview of the professionals’ level of understanding about the new ways of working in the clinical setting. Hence, a new dental care protocol was developed based on scientific evidence and practices already adopted by most dental professionals, with a focus on the procedures that are not yet massively implemented. The actions of dentists need to be reorganized in the following situations: before appointment (Figure 2), handling of the operative area (Figure 2), and use of PPE (Figure 3 and 4).
|
Study |
Protocol |
|
Peditto., et al. 2020 Italy |
1. Every patient should be treated as a possible carrier of the virus; |
|
2. Elective procedures must be postponed; |
|
|
3. The consultations must be scheduled in order to admit only one patient at a time in the clinical areas, without the presence of companions; |
|
|
4. The professional should take a shower before going to the office and then, shave facial hair, short nails and avoid using accessories; |
|
|
5. Wash hands before and after each procedure, avoiding touching your face; |
|
|
6. Disinfection of surfaces; |
|
|
7. Use of PPE in clinical practice; |
|
|
8. Goggles and visors must be disinfected with 70% ethyl alcohol before and after each treatment; |
|
|
9. Patient care is carried out in 2 stages: Prior screening (telephone, message, texts) and care (treatment). |
|
|
a. In the case of postponable procedures, the patient must be informed about preventive measures and prescription of medications. |
|
|
b. In the service, the patient is invited to rinse for 30 s with a 1% hydrogen peroxide solution or with 1% povidone iodine and then with 0.2/0.3% chlorhexidine for 1 min. |
|
|
Pereira., et al. 2020 Brazil |
1. The patient may be infected even without symptoms (The patient must be treated as an imminent danger of infection); |
|
2. All elective and non-essential procedure must be postponed |
|
|
3. Use of teleodontology (calls, text messages) for prior assistance. If necessary, the professional will advise and prescribe medication; |
|
|
4. Daily monitoring of the health team and patient temperature; |
|
|
5. Use of PPE; |
|
|
6. Avoid crowding, having only 1 patient in the waiting room; |
|
|
7. Before treatment, rinse with 1% or 1.5% hydrogen peroxide or 0.2% povidone; |
|
|
8. To minimize aerosol production, dentists should use manual instrumentation, high volume saliva ejector and dental dam during treatment; |
|
|
9. Intraoral radiographs should be avoided as they can induce cough. |
|
|
Giudice et al, 2020 Italy |
1. Inform patients of the procedures for accessing the dental office. |
|
2. Carry out a preliminary telephone triage upon patient access to the office in order to assess whether: |
|
|
a. The patient who is entering the office has symptoms of SARS-CoV-2 infection; |
|
|
b. Has come into contact with potentially infected people; |
|
|
c. Has been in areas with high risk of infection. |
|
|
3. Any suspicious case will be reported to competent health authorities for further investigation. |
|
|
4. Only schedule an appointment in the dental office if the patient cannot be deferred or in urgent cases and according to the equipment and disposable materials available. |
|
|
5. Assess the actual need for dental intervention before planning visits of the most vulnerable subjects (elderly or patients with respiratory, cardiovascular, or immune system diseases, etc |
|
|
6. Avoid crowding by spreading appointments over time, maintaining distance in the waiting room and/or in the operating rooms (minimum safety distance of 2 m with a stay of less than 15 min). |
|
|
7. Arrange entry into the operating rooms of individual patients and a single companion for minors, without overcoats, electronic devices, and bags, which must be left in the waiting room. |
|
|
8. Ensure that hand sanitizer is available to patients and companions |
|
|
9. Always allow fresh air in between one patient and another, and frequently in the waiting room |
|
|
10. Manage all material that comes into direct or indirect contact with the patient according to the proper disposal techniques |
|
|
11. Always use PPE. Check integrity of PPE |
|
|
12. Scrupulously observe hand hygiene |
|
|
13. Remove potentially contaminating objects from waiting rooms and operating rooms |
|
|
14. Regularly sanitize common and operational areas, non-medical furnishings and equipment, and surfaces accessible to the public |
|
|
15. Place protections on points of sale (POSs), keyboards, etc. and change them after each use. A single-use protection could be a disposable barrier (plastic film or cover) that must be replaced after every use. |
|
|
16. Protect the surfaces of all equipment and instruments with single-use disposable barriers and dispose of the protections among the special waste after use. |
|
|
17. Arrange only strictly necessary material on the surfaces of operating areas. |
|
|
18. Clean the operative surfaces with hydroalcoholic disinfectants at concentrations above 60%. |
|
|
19. Wear a uniform with long sleeves and shoes, and avoid exposed body parts. |
|
|
20. Wear a disposable lab coat/overcoat. |
|
|
21. It is also suggested that the patient mouth-rinse for 30 s with a 1% solution of hydrogen peroxide (1 part at 10-volume/3% hydrogen peroxide and 2 parts of water) or with 1% iodopovidone. |
|
|
22. Give preference to extra-oral radiological examinations over intra-oral ones to avoid the stimulation of coughing or vomiting. |
|
|
23. Replace and sterilize the high- and low-speed hand-pieces after each use between one patient and the next; |
|
|
24. When possible, apply a rubber dam to reduce possible aerosol production |
|
|
Passareli., et al. 2020 USA |
Anamnesis questionnaire: |
|
1. Did you have fever? |
|
|
2. Did you have any respiratory symptoms or problems? |
|
|
3. Did you have conjunctivitis? |
|
|
4. Have you or any member of your family had contact with a patient with a positive diagnosis for COVID-19 in the last 14 days? |
|
|
5. Have you or any member of your family had contact with a patient with a suspected symptom of COVID-19 in the last 14 days? |
|
|
Meng., et al. 2020 China
|
1. Wash hands frequently; |
|
2. Total disinfection of surfaces; |
|
|
3. Appropriate PPE to the work team (for type B infectious diseases); |
|
|
4. Avoid or decrease aerosol generating procedures; |
|
|
5. Prior screening, with body temperature measurement; |
|
|
6. Anamnesis containing symptoms history, contact with sick people and recent travel history; |
|
|
7. Antimicrobial mouthwash before procedures; |
|
|
8. Give preference to extraoral radiographic exams (intraoral exams stimulate increased salivation); |
|
|
9. Use of rubber dikes for total isolation; |
|
|
10. Use of high-power suction; |
|
|
11. Postpone non-urgent invasive procedures. |
Table 3: Protocols assessed in protocol studies selected.
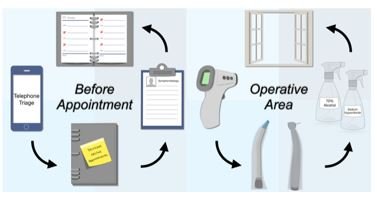
Figure 2: Flow diagram of Before appointment and Protective area measures.

Figure 3: All steps to clothe the personal protective equipment (adapted from Sales-Peres, 2021 [36]).
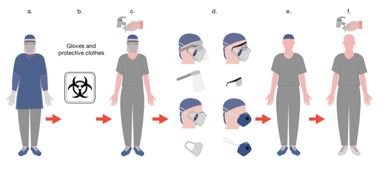
Figure 4: All steps to remove the personal protective equipment (adapted from Sales-Peres, 2021 [36]).
Before dental care, it is essential to take preventive and diagnostic measures to optimize care:
Operative area: The patient's temperature should be measured before entering the room. In the operating environment, protectors should be used in the dental chair, instrument bench, and turbines. This protection must be changed after each patient's care. All surfaces must be disinfected - soaking the surfaces with a bleach containing 5.25% - 8.25% sodium hypochlorite for at least 1 min or spraying them with 70% alcohol [36] - after contact with each patient. High-power suction and absolute insulation with a rubber sheet should be used whenever the procedure allows. The ventilation of the operating room must be performed after each appointment.
PPE use: Complete PPE must be used for all procedures:
The sequence of wearing and deparmenting are illustrated in figures 3 and 4 (adapted from Sales-Peres, 2021 [37]).
Our study has some limitations. Due to the need to rapidly obtain sufficient evidence about the risk groups and disease therapy, we were unable to collect enough scientific evidence regarding other preventive methods. Solutions used for disinfection and those for mouthwash are still being utilized empirically in order to obtain the best results.
The strength of our study is the formulation of a dental care protocol based on scientific evidence and the current knowledge, practices, and perception of professionals, making the present study extremely strong.
We concluded that dentists can play an important role in preventing and interrupting the COVID-19 transmission chain. Assuming responsibilities and performing correct procedures to reduce the undesirable spread of infectious diseases and those in accordance with the appropriate safety protocols for the prevention of COVID-19 are the basic measures that must be taken. The clinical care protocol in dentistry should be adopted for all dentists to avoid biological risk.
The authors are grateful to University of São Paulo, São Paulo Research Foundation (FAPESP; grant nº. 18/25934-0) and Coordination for the Improvement of Higher Education Personnel (CAPES - Finance Code 001).
None.
Citation: Silvia Helena de Carvalho Sales-Peres., et al. “Coronavirus Disease 2019 Biological Risk and Clinical Care Protocol in Dentistry: A Systematic Review”. Acta Scientific Dental Sciences 5.5 (2021): 28-43.
Copyright: © 2021 Silvia Helena de Carvalho Sales-Peres., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.
