Apurva Kabra* and Girija Wagh
Department of Obstetrics and Gynecology, Bharati Vidyapeeth Deemed University, Pune, India
*Corresponding Author: Apurva Kabra, Apurva Kabra, Junior Resident, Department of Obstetrics and Gynecology, Bharati Vidyapeeth Deemed University, Pune, Maharashtra, India.
Received: August 29, 2024; Published: September 10, 2024
Citation: Apurva Kabra and Girija Wagh. “Case Report on Painless Torsion of Non Gravid Myomatous Uterus". Acta Scientific Women's Health 6.10 (2024):07-09.
Uterine torsion is defined as rotation of more than 45 degrees around the long axis of the uterus. Uterine torsion is an uncommon event but extremely rare with only 25 cases reported in last 20 years. Most of the torsion is seen in gravid uterus and nonpregnant uterine torsion is a rarity.
Here is the case report of painless torsion of a non-gravid uterus with multiple intramural and sub serosal fibroids in 46 years old parous, perimenopausal woman. Mrs. A came with an incidental finding on sonographic evaluation of multiple uterine leiomyomas. She was asymptomatic but after probing revealed vague pain and heavy menstrual bleeding which she took as normal. In view of anemia acquired due to menorrhagia it was decided to do hysterectomy and was posted for total hysterectomy after anemia correction. To our surprise, after opening the abdomen near to complete torsion of the uterus was noticed. Untwisting of myomatous uterus was done and total abdominal hysterectomy with bilateral salpingectomy was performed. The patient's postoperative course was uneventful. It was surprising to note that the patient was asymptomatic despite such a torsion.
Keywords: Uterine Torsion; Painless; Myomatous; Non Gravid; Hysterectomy
Uterine torsion is defined as a rotation of more than 45 degree around the long axis of the uterus [1]. Although uterine torsion is rare, it has been reported in women of all ages from premenarcheal to postmenopausal stages. Gravid uterus accounts for most of the reported cases and uterine torsion in non-gravid women is extremely rare. Multiple case reports have described torsion either in the gravid uterus [2] or in postmenopausal women [3], yet rarely in the non-gravid, premenopausal uterus. Only 25 cases of uterine torsion in non-gravid women have been reported in English literature available on PubMed over last 20 years [1].
To the best of our knowledge, there remains only a single case of uterine torsion in a premenopausal non-gravid woman in the literature, described in 1935. Although it is difficult to diagnose due to its rarity and nonspecific symptoms and laboratory data, it can be life threatening. Here, we report a case of painless torsion of non-gravid myomatous uterus.
Performed at tertiary care center, Bharati Hospital, Pune, India (case report).
Case Report
Mrs. A, 46 years old parous, perimenopausal woman presented with an incidental finding on sonographic evaluation of a large uterus with multiple uterine leiomyomas for further guidance of clinical action.
Her previous menstrual cycles were regular, with no history of passage of clots, but on probing further she revealed increase bleeding with flooding in the recent few months which she took as normal perimenopausal occurrence. Her obstetric history revealed three uneventful vaginal births. She had no history of diabetes mellitus, hypertension, tuberculosis, bleeding disorders, blood transfusion in past. Personal and family history were noncontributory.
On examination she was vitally stable and abdominal examination revealed a palpable mass corresponding to 12-14 weeks gravid uterus. The mass was arising from the pelvis, of size 12cm x 10 cm, firm to hard in consistency with restricted mobility and vaginal assessment confirmed the pelvic assessment findings with no additional pathology. Working diagnosis corroborated by the ultrasound was confirmed to be uterine fibroid.
Her laboratory investigations were normal. Ultrasonography revealed two large leiomyomas:
Pre anesthetic checkup was done. Echo cardiogram suggested -ST flattening and further cardiac work up was done. It came to be normal, and she was fit for surgery.
As she was asymptomatic, posted for elective total abdominal hysterectomy and bilateral salpingectomy. The diagram below depicts the intraoperative findings (Figure 1).
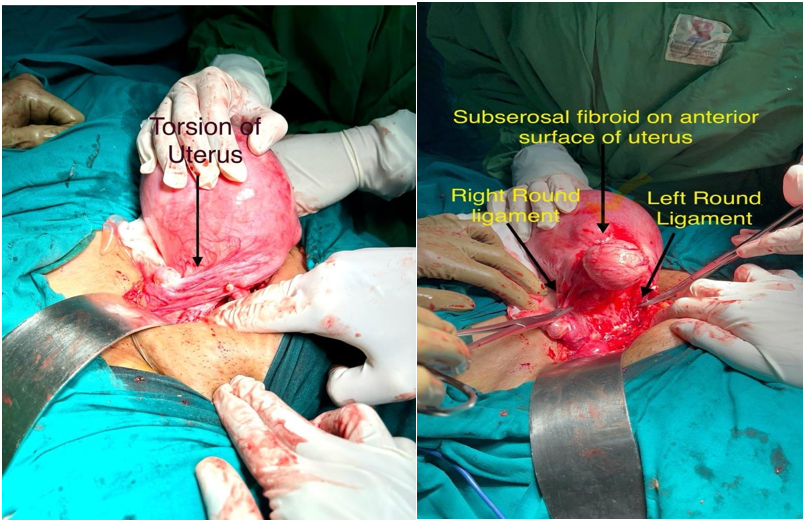
Figure 1: A. Intraoperative picture with torsion. B. After detorsion of the uterus.
Intra operatively findings of torsion of uterus at the level of internal os. Anterior fundal sub serosal fibroid, pulled up round ligaments and whole of posterior uterus was occupied by fibroid and hence distorted anatomy of uterus and surrounding structures noted.
Torsion of uterus corrected, identified structures correctly- round ligament along with Tubo-ovarian ligament clamped together- cut- ligated. Congestion noted at Tubo-ovarian ligaments due to torsion.
Further the surgery was completed with total abdominal hysterectomy with bilateral salpingectomy. A cut open specimen revealed 12cm x 10 cm fundal intramural fibroid with hemorrhagic areas seen. Specimen sent for histopathological examination. Vault closure and suspension done. Hemostasis confirmed and abdomen closed in layers. The procedure was uneventful. Intra and post operatively broad-spectrum antibiotic coverage was done. The post operative phase was uneventful.
Torsion of a nongravid uterus is extremely rare, and most of the reported cases involve a large myomatous uterus The uterus may rotate due to its weight, thus exerting traction on the uterus. Other conditions reported in cases of torsion of a nongravid uterus are a normal-sized uterus accompanied by a large ovarian cyst and a uterine anomaly in combination with complete cervical agenesis.
The incidence of uterine torsion cannot be clearly established because of following reasons,
The cases could to be categorized as
They can also be categorized according to duration of symptoms
The exact cause is still unclear though several conditions associated with it structural anomalies that distort pelvic anatomy, such as pregnancy, uterine fibroids, ovarian cysts [2] and adnexal tumors, and ligamentous laxity in the pelvis [2].
Uterine torsion is a rare condition that can occur in women with fibroid uterus while is commoner in gravid uterus. It is characterized by the twisting of the uterus on its own axis, leading to a variety of symptoms including severe abdominal pain, nausea, and vomiting and can be symptomatic probably due to gradually or non-acute torsion. It can pose a challenge at surgery and the correct anatomy should be established before starting the surgery. Imaging should be able to guide the surgeon but needs strong suspicion. Early diagnosis and prompt surgical intervention are crucial in order to prevent complications such as ischemia, necrosis, or even rupture of the uterus. In this case report, the patient presented with atypical symptoms and a delay in seeking medical attention, resulting in a more challenging surgical procedure. The case highlights the importance of considering uterine torsion as a differential diagnosis in women with fibroid uterus who present with acute abdominal pain. It also emphasizes the need for increased awareness among healthcare professionals and patients regarding this rare but potentially life-threatening condition. Further research is needed to better understand the risk factors, pathophysiology, and optimal management strategies for uterine torsion in women with fibroid uterus. In the meantime, it is crucial for healthcare providers to maintain a high index of suspicion and promptly investigate and manage any suspected cases to prevent adverse outcomes.
No any financial interest or any conflict of interest exists.
Copyright: © 2024 Apurva Kabra and Girija Wagh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff







