Sujnanendra Mishra1* and Swadhin Kumar Mishra2
1Senior Consultant, Swaraj Hospital and Research Institute, Bolangir, Odisha, India
2Consultant, Swaraj Hospital and Research Institute, Bolangir, Odisha, India
*Corresponding Author: Sujnanendra Mishra, Senior Consultant, Swaraj Hospital and Research Institute, Bolangir, Odisha, India.
Received: July 29, 2024; Published: August 27, 2024
Citation: Sujnanendra Mishra and Swadhin Kumar Mishra. “When Family Ties Uncover Unusual Pathology: Microperforate Hymen a Case Report". Acta Scientific Paediatrics 6.9 (2024):28-30.
In this case report, we discuss a 12-year-old girl who presented with fever, abdominal pain, recurrent vulval discharge, and dysuria. Upon examination, she was diagnosed with a microperforate hymen and pyocolpos. Notably, her mother had a history of imperforate hymen. Treatment involved intravenous antibiotics and hymenotomy, resulting in drainage of 150 cc of purulent fluid. This case highlights the critical importance of thorough genital inspection and consideration of hymenal anomalies in the differential diagnosis for girls experiencing recurrent dysuria, fever, and prolonged vulvar discharge.
Keywords: Dysuria; Fever; Outpatient Department (OPD)
Introduction: The hymen, a membranous remnant, forms at the junction between the Sino-vaginal bulbs and the urogenital sinus. Typically, it perforates during embryogenesis and remains open at birth. However, various hymeneal abnormalities exist, including imperforate, micro perforate, annular, septate, cribriform (sieve-like), and navicular (boat-like) types. Imperforate hymen results from the inferior end of the vaginal plate failing to canalize, with an incidence of approximately 1 in 1000 to 2000 females. Rarely, sporadic cases of imperforate hymen occur in multiple family members [1].
A 12-year-old girl presented to our outpatient department (OPD) with a history of fever and dysuria, which had been treated with various antibiotics for over a year. She also complained of recurrent foul-smelling discharge from the vulva for approximately 3 months. Three days prior, she experienced acute abdominal pain and was admitted to a nearby hospital. Subsequently, she sought further management at our hospital. Family history was quite remarkable. Her mother underwent a surgery at the age of 18 to address an imperforate hymen with Hematocolpos and hematometra.
The patient appeared average in build and had no signs of pallor, icterus, cyanosis, pedal edema, or generalized lymphadenopathy. Vital signs were within normal limits (pulse rate: 96 beats per minute, blood pressure: 112/76 mmHg, temperature: 98.8°F). Chest and cardiovascular examinations were normal. Secondary sexual characteristics were not developed. On local examination, external genitalia appeared normal. The urethral meatus was normal, apparently intact hymen without any bulge, a tiny pin point hole was seen at 6 ‘o clock position. Per rectal examination revealed a cystic mass above the anal verge through the anterior rectal wall. When pressing the mass per rectum, a foul-smelling discharge emerged from the hymenal hole.
Hemoglobin: 10.4 g/dL, Total leukocyte count: 19,670/microliter, Absolute Neutrophil count: 74%, Erythrocyte sedimentation rate: 61 mm. Platelet count: 256,000/microliter. Random blood sugars: 108 mg/dL. Liver and kidney function tests were normal. Urine routine microscopy and culture sensitivity were unremarkable. Combined abdominal-perineal sonography image showed cystic mass 9 cm X 9 cm with internal echoes (Figure 2). Bilateral ovaries were normal.

Figure 1: Apparently intact hymen without any bulge with a tiny pin point hole at 6 ‘o clock position.
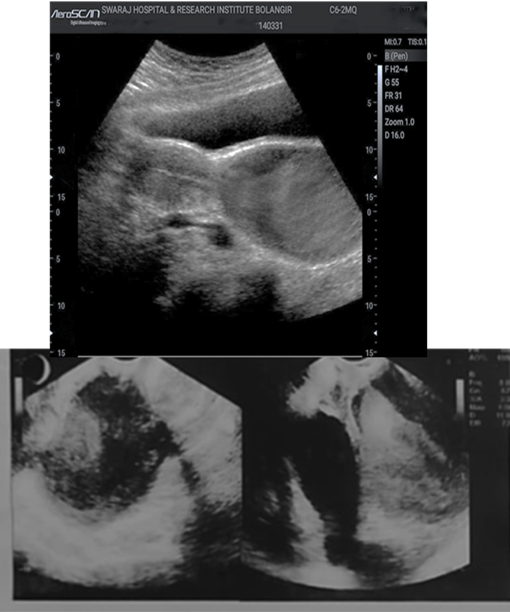
Figure 2: Combined abdominal-perineal sonography image showing cystic mass 9 cm X 9 cm with internal echoes.
The patient was admitted and started on antibiotics and analgesics. Under anesthesia, a needle was inserted through the hymen, and pus was aspirated for culture sensitivity. A cruciate incision was made in the hymen, draining approximately 150 mL of pus. Hymenectomy was performed, and the edges of the vaginal mucosa were sutured at the introitus. Betadine vaginal wash was administered, ensuring hemostasis. The patient tolerated the procedure well. The catheter was removed on postoperative day 2, and she was discharged in stable condition on postoperative day 3. Follow-up after two weeks revealed a healthy wound.
Hydrometrocolpos and Hematocolpos, as well as hematometra, are conditions that can arise in individuals with obstructions in the female genital tract due to malformations. These conditions manifest during two distinct life stages, linked to the endometrium’s functional characteristics: either during the newborn-infancy-childhood phase or at the onset of puberty [2].
In newborns and young children, the genital secretion caused by endogenous estrogen stimulation accumulate within the obstructed vagina, known as hydrocolpos, is. Conversely, at puberty, the endometrium undergoes periodic bleeding. However, due to malformations, this can lead to a blockage of the normal menstrual flow, resulting in ‘cryptomenorrhea,’ along with hematocolpos and hematometra [3].
Imperforate hymen is a rare reproductive tract anomaly, affecting around 0.1% of newborn females. Few case reports highlight the familial occurrence of imperforate hymen in a child, her mother, and her mother’s monozygotic twin [3]. Micro perforate Hymen (MH) is a partially obstructive hymenal anomaly. Symptoms vary among individuals, possibly depending on the diameter of the hymen opening. Girls born with such anomaly may remain asymptomatic during infancy and childhood. Prior to puberty they can present with Hydro/muco/pyocolpos. At puberty, some young women with MH have a normal menstrual cycle with light flow, while others experience irregular postmenstrual spotting due to incomplete drainage of menstrual blood products and later dyspareunia, inability to have vaginal intercourse, The diagnosis of MH at times be delayed until later in adulthood when patients present with infection (pyocolpos), infertility or significant dyspareunia. Premenarchal girls with MH are at increased risk for recurrent urinary tract infections (UTIs). Two hypotheses explain this: UTI due to urinary retention caused by partial obstruction of the urethra by entrapped vaginal secretions (e.g., hydrocolpos or mucocolpos), or bacterial ascent from the vaginal canal via micro perforation in the hymen. MH patients are also at risk for recurrent vulvovaginitis and ascending pelvic infection. Pyocolpos, characterized by an obstructed pus-filled vagina, can occur in MH cases. Symptoms include abdominal pain, fever, UTI, urinary retention, leukorrhea, and vulvovaginitis. Ultrasound imaging reveals a large dilated cystic structure with low-level internal echoes and fluid-debris levels. Pyocolpos results from bacterial colonization and invasion of entrapped vaginal secretions, partially obstructed by the small MH opening. Urgent surgical consultation is necessary to prevent complications like vesicovaginal fistulae, vaginal mucosal destruction, and sepsis.
Thorough routine genitourinary examination of the external genitalia is essential in girls of all ages from birth through the onset of menarche by the clinicians can prevent the significant delays in diagnosis, misdiagnosis, and morbidity associated with the condition. ³ Early Diagnosis and management could have prevented infection and related morbidity. This case highlights the importance of evaluating female members of the affected patients. Outcome after surgery of imperforate hymen is excellent. If findings on an appropriate preoperative evaluation are normal without other Mullerian abnormality, a patient can be reassured that her genital tract is otherwise normal.
This research was conducted without external funding.
The authors declare no conflicts of interest or competing interests related to this study.
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of Swaraj Hospital & Research Institute. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent was obtained from the patient for her participation in this study. She was informed about the purpose of the study, potential risks, and benefits, and voluntarily agreed to participate.
The patient provided written consent for the publication of her case details, including clinical history, imaging findings, and surgical management.
The data and materials supporting this study are available upon request from the corresponding author.
No specific software application or custom code was used in this study.
Copyright: © 2024 Sujnanendra Mishra and Swadhin Kumar Mishra. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff







