Pal Rahul, Rathod Harshala, Karve Sanjana and Gokarn Nishit Suhas*
Department of Veterinary Surgery, The Progressive Pet Clinic, India
*Corresponding Author: Gokarn Nishit Suhas, Department of Veterinary Surgery, The Progressive Pet Clinic, India.
Received: September 05, 2024; Published: September 26, 2024
Citation: Gokarn Nishit Suhas., et al. “A Rare Case of Uterine Intussusception in a Cat and its Successful Surgical Management”. Acta Scientific Veterinary Sciences 6.10 (2024): 17-20.
Uterine intussusception in cats is a rare but potentially life-threatening condition that requires prompt diagnosis and surgical intervention. This case report describes the clinical presentation, diagnosis, surgical management and outcome of uterine intussusception in a domestic shorthair cat. The importance of recognizing this condition and the surgical techniques employed for successful correction are discussed, with a review of relevant literature.
Keywords: Uterine Intussusception; Queen; Dystocia
Uterine intussusception, though rare in veterinary practice, can occur in cats and presents significant diagnostic and therapeutic challenges. Intussusception, a clinical emergency for the intestines, is commonly characterized as the telescoping of one part with the other part of the intestine [1]. Telescoping or intussusception of an organ disrupts arterial blood supply, resulting in cyanosis and necrosis. Surgical excision of the afflicted area is the preferred therapeutic option [2,14]. The most common clinical indications of uterine intussusception include unproductive contractions and abdominal discomfort [11]. However, there is no evidence in the literature that uterine intussusception is a cause of dystocia. This case report is the first to identify and record in India as uterine intussusception as a cause of dystocia in a primiparous cat and its successful surgical management. This report aims to contribute to the limited body of knowledge on uterine intussusception in cats, emphasizing the importance of timely surgical intervention.
A 4-year-old, primiparous Domestic Short Hair breed cat weighing 4.4 kg, was presented with a history of full-term pregnancy with 1 non-viable fetus delivered 8 hours ago. After the first delivery, the queen showed signs of straining, acute abdominal tenderness, lethargy and anorexia. On clinical examination the rectal temperature was 102.2 °F with Body Condition Score (BCS) of 4/9. The cat was very restless with abdominal discomfort pain, hyperpnoea (64 breath/min), tachycardia (226 beats/min) with congested conjunctival mucus membranes, capillary refill time (2 sec) and normal lymph nodes. On physical examination revealed a palpable abdominal mass and signs of discomfort upon palpation.
Blood samples were collected for haematological and biochemical analyses in which complete blood count (CBC) were normal in range except mild leucocytosis 23k/uL using haematological analyser (ProCyte Dx, IDEXX) while serum blood urea nitrogen, serum creatinine and serum glutamic pyruvic transaminase were also normal in range using biochemical analyzer (Dri-chem Nx500i, Fujifilm). Mild leucocytosis was evident in the hemogram indicating possible onset of infection. Transabdominal ultrasonography (GE healthcare Versana active, 6.5 MHz convex transducer) revealed a tubular, layered structure suggestive of intussusception and a dead fetus. After stabilizing the patient and acquiring informed consent an exploratory laparotomy was performed, and an ovariohysterectomy was recommended.
Preoperatively premedicated with antibiotics 20mg/kg amoxicillin-clavulanate (Amoxirum forte; Virbac), analgesics buprenorphine @ 0.02mg/kg (Buprigesic; Neon Laboratories) and fluid therapy @ 20ml/kg. Pre-anesthetic medication tiletamine and zolazepam @ 5mg/kg (ZoletilTM 50, Virbac) administered intramuscularly. After seven minutes general anaesthesia was induced by intravenous injection of 5 mg/kg propofol (Neorof; Neon Laboratories Limited). After endotracheal intubation with ET tube No. 4, the anaesthesia was maintained with Isoflurane (Sosrane; Neon Laboratories Limited) on a non-rebreathing system. The mid-ventral abdomen i.e. surgical site was clipped, cleaned and scrubbed with 7.5 per cent povidone iodine solution and sterile drape was applied exposing the surgical site aseptically.
The cat was placed in a dorsal recumbency and ventral midline incision extending from caudal to the umbilicus 5-10 cm towards the pubis was made. A stab incision was made on the linea alba near the umbilicus and extended caudally towards the pubis to access the abdominal cavity. On exteriorization it was observed (Figure 1) that complete right uterine horn had telescoped into the uterine body and left uterine contained a non-viable foetus that was obstructed due to intussusception. The affected uterine segment was inspected for viability. Despite mild congestion, the tissue was deemed viable. The intussuscepted segment was gently reduced manually, restoring normal anatomical alignment [Figure 2]. Ovariohysterectomy was performed to prevent recurrence and potential complications. The abdominal cavity was lavaged with warm saline, and the abdominal incision at the linea alba was closed by a simple interrupted continuous suture pattern using PDS No. 3-0. Subcutaneous layers and skin layers were closed by simple continuous suture pattern using the Monocryl size no. 4-0. The surgical site was packed with sterile gauze piece and taped.
The cat was monitored closely postoperatively for signs of infection and pain. Analgesics and antibiotics were continued as per the protocol. The cat recovered uneventfully, with normal activity levels and appetite returning within a few days. Follow-up examinations at two weeks and one month post-surgery confirmed complete recovery.
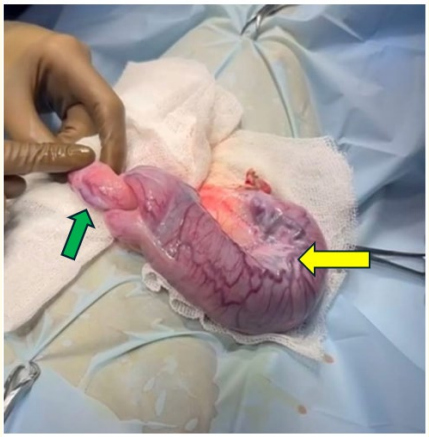
Figure 1: Uterine intussusception in which yellow arrow indicates gravid horn with non-viable fetus and green arrow indicates non-gravid horn intussuscepted in uterine body.
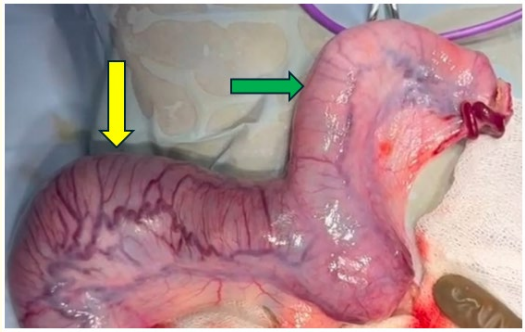
Figure 2: Uterine horns after correcting uterine intussusception yellow indicates gravid uterine horn with non-viable fetus and green arrow indicates non-gravid uterine horn after correction.
Uterine intussusception is an uncommon disorder with few known instances globally. Unfortunately, there is no reliable estimate of its occurrence in cats [10]. Uterine intussusception in cats is an uncommon condition with two reported cases in the literature [9,13]. Although the exact cause of the condition is unknown, it is thought to be related to the uterine tubular structure and contraction ability [3,2], nutritional deficits (e.g., calcium insufficiency), post-parturition physiological factors (e.g., uterine involution, regeneration of the uterine tract, and hormonal changes), and pathological factors (e.g., prolonged dystocia) appear to be risk factors for uterine intussusception [7,8,10,16]. The large litter number resulted in high distention of uterine broad ligaments leading to uterine body intussusception to occur dystocia [13]. One of the possible causes of uterine intussusception, is presence of an unequal number of fetuses in both uterine horns (Two in right and one in the left horn) and hyperactive movement of the animal [4]. In the present case the cat presented as dystocia which was further diagnosed as uterine intussusception.
The clinical symptoms associated with uterine intussusception in dogs were abdominal discomfort due to the hyperactive movement of the animal [2,6]. A history of high temperature (40°C) along with hyperpnoea and tachycardia were in agreement with the reports of uterine torsion and intussusception [6,15]. In previously described cases, the symptoms included weakness, acute abdominal pain, lethargy, anorexia, hyperpnea and tachycardia [9,13]. In the reported instance, the majority of the symptoms were observed and reported by the owner.
Routine diagnostic tools, such as radiography and ultrasonography, cannot detect uterine torsion or intussusceptions [2,14,15]. Only exploratory laparotomy can reveal both conditions [2,12]. In present case ultrasonography was opted first to detect the fetal heart rate and accidentally noticed the tubular, double layered structure consistent with intussusception and a non-viable fetus.
In the present case study, after invaginating the intussuscepted uterine segment during ovary-hysterectomy, it was observed that external wall of the uterine horn slightly necrosed and congested due to involvement of vascular stasis because of uterine intussusception. This scenario may encourage devitalization of the afflicted section, as demonstrated by cases of intestinal intussusception [5].
As a result, it was recommended to do an ovario-hysterectomy as soon as possible after conservative treatment failed to minimize invagination in order to prevent ischemia processes that would endanger the patient’s overall health.
Thus, this clinical case report is a rare and first finding of uterine intussusception in a gravid primiparous queen causing a dystocia.
Uterine intussusception, though rare, should be considered in the differential diagnosis of acute abdominal pain in female gravid cats. Surgical intervention exploratory laparotomy and ovariohysterectomy, is essential for definitive treatment and prevention of recurrence. This case report adds to the limited literature on uterine intussusception in cats and underscores the need for prompt diagnosis and surgical management.
We extend our gratitude to the surgical team at The Progressive Veterinary Clinic for their expertise and dedication in managing this complex case.
The authors declare that they do not have any conflict of interest.
Copyright: © 2024 Gokarn Nishit Suhas., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff







