Gurleen Kaur1* and Mostafa Zein2
1Veterinarian at Crown Vets Pet Clinic and Diagnostics, Jalandhar, Punjab, India
2Veterinarian at Harmony Vet Clinic, International City, Dubai
*Corresponding Author: Gurleen Kaur, Veterinarian at Crown Vets Pet Clinic and Diagnostics, Punjab, India.
Received: July 25, 2024; Published: August 25, 2024
Citation: Gurleen Kaur and Mostafa Zein. “Surgical Management of Foreign Body in a Cat”. Acta Scientific Veterinary Sciences 6.9 (2024): 24-26.
A four-year-old Ling-Ling Siamese cat was presented with history of ingesting a rubber-band. The cat had been experiencing anorexia, lethargy and severe vomition past one day. Ultrasonographic examination revealed acoustic shadowing indicating foreign body lodged in gastrointestinal tract. Following induction of general anaesthesia, the patient underwent enterotomy to extract a rubber band, which was accomplished successfully.
Keywords: Cat; Linear Foreign Body; Enterotomy; Anaesthesia
Gastro-intestinal foreign body obstructions result in disruption of fluid-balance, disturbs acid-base equilibrium, and hence serum electrolyte concentrations because of increased secretion and retention within the gastrointestinal tract, which gets exacerbated by persistent vomition and hence reduced intake of fluids and nutrients. Cats are recognized for their opportunistic feeding behaviour, leading to frequent ingestion of foreign bodies. Foreign bodies commonly become lodged in the jejunum, ileum, and duodenum. The diagnosis of intestinal foreign bodies can be made by using contrast radiographic techniques, ultrasonographic examination and endoscopy [1].
A four-year-old Ling-Ling Siamese cat was presented with history of ingesting a rubber-band. The cat had been experiencing anorexia, lethargy and severe vomition past one day. Upon further clinical examination, the cat presented with lethargy, dehydration, and demonstrated discomfort upon abdominal palpation. Complete blood count and serum biochemical analysis revealed values that were within normal ranges. The ultrasonographic examination suggested the presence of a foreign body in the intestinal and gastric regions, leading to subsequent pyloric obstruction (Figure1.). Exploratory laparotomy was recommended to confirm and treat the suspected foreign body after proper stabilisation. Following general anaesthesia, enterotomy was performed.
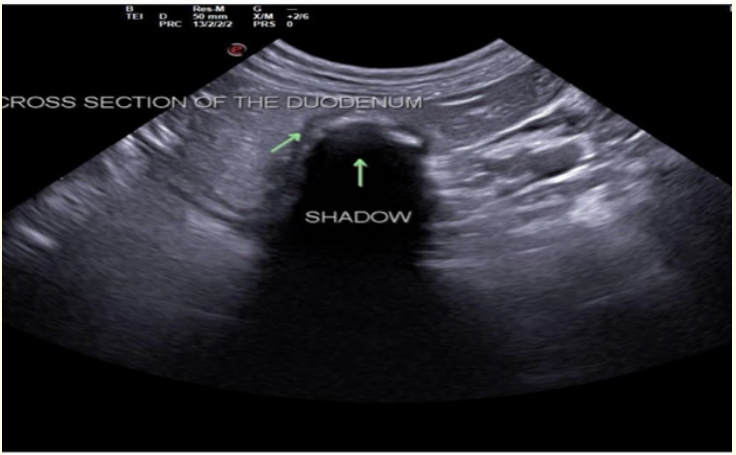
Figure 1: Acoustic shadowing below the stomach.
Preoperatively, animal was stabilised with fluid therapy, Infusion Ringer lactate @200ml I/V and Infusion metronidazole@15mg/kg I/V.
LingLing was sedated with dexmedetomidine@40micrograms/ kg, Buprenorphine@0.01milligrams/kg, ketamine@5milligrams/ kg bodyweight intramuscularly. The anaesthesia was sustained by administering a combination of inhalant isoflurane and oxygen.
The surgical site was prepared aseptically. A ventral midline celiotomy was performed. The intestines were exposed at the surgical site. Distended loop of intestine was noticed at the duodenum level (Figure 2). The foreign body was palpated at the duodenal level, atraumatic clamps were applied on the proximal and distal end, and a linear incision was made in healthy-looking tissue, distal to foreign body (Figure 3).
The foreign body (rubber-band) was retrieved, and cleaning of intestinal segment was performed with normal saline solution. Enterotomy incision was closed with inverted double layer pattern cushing’s followed by lembert suture pattern, using 3-0 Polydioxanone (monofilament absorbable suture material) and omentum was distributed over the suture line before closing the abdomen. Before closure, entire tract was examined for perforation and reduced vascular perfusion. Abdominal lavage was conducted using warm normal saline, followed by standard abdominal closure procedures [2].
Cat was kept off-fed for three days and I/V fluid infusion of ringer Lactate@200ml/kg, along with I/V infusion of metronidazole@15mg/kg, amoxicillin@0.1ml/kg, Cerenia@0.1ml/ kg was continued for a week.
Soft diet was started on fourth day after surgery to enhance the motility of intestine. Lingling recovered uneventfully.
Based upon history and clinical signs exhibited by the animal, ultrasound of abdomen was performed.

Figure 2: Distended intestinal loop.
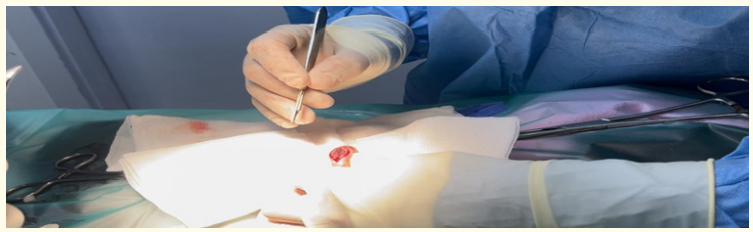
Figure 3: Linear incision given on intestine.
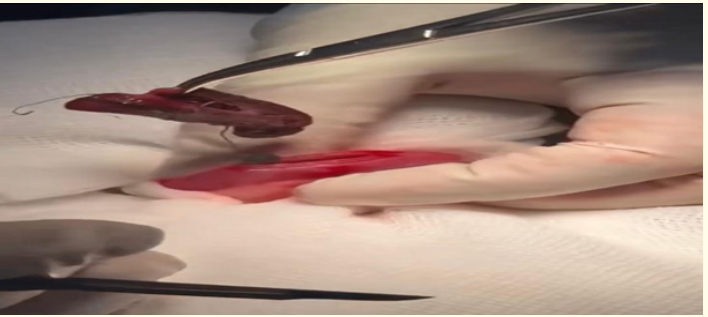
Figure 4: Foreign body retrieved.
The ultrasonographic examination highly suspected a gastric and an intestinal foreign body with subsequent pyloric obstruction. Therefore, an enterotomy was performed, which resulted in successful retrieval of the foreign body (rubber band) figure4. Cat recovered fully without any uneventful complications [3].
Gastrointestinal obstruction results from complex interactions involving systemic and local factors, some of which remain poorly understood. This condition can lead to severe complications such as hypovolemia, toxaemia, fluid, acid-base, and electrolyte imbalances, which poses significant health risks.
Accumulation of fluids occurs due to two primary reasons: retention of ingested fluids and increased secretion in the upper gastrointestinal tract. Factors contributing to impaired solute absorption include lymphatic and venous congestion, elevated osmolality within the intestines, and a decreased turnover rate of enterocytes.
Local hypersecretion exacerbates these issues, and prolonged obstruction lasting 24 hours or more can render the dilated intestine incapable of effectively absorbing fluids. These processes highlight the critical importance of timely management of gastrointestinal blockages to prevent potentially life-threatening complications.
The volume of fluid in the intestinal lumen increases in direct proportion to the length of the obstruction. In cases of complete blockages in the upper part of the intestine, a substantial quantity of secretions and ingested fluids cannot reach the mucosal surfaces of the jejunum and ileum for absorption. Conversely, in distal intestinal blockages, fluids may undergo reverse peristalsis to reach an unaffected, non-distended segment of the intestine where normal absorption occurs.
Copyright: © 2024 Gurleen Kaur and Mostafa Zein. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff







