Camarena J*, Almonte C, Vicente E, Sánchez W, Rodríguez J and Santana Y
Digestive Endoscopy Unit, Obstetrics and Gynecology Center, Santo Domingo, Dominican Republic
*Corresponding Author: Camarena J, Digestive Endoscopy Unit, Obstetrics and Gynecology Center, Santo Domingo, Dominican Republic.
Received: August 01, 2024; Published: September 06, 2024
Citation: Camarena J., et al. “Button Batteries in the Upper Digestive Tract: A New Challenge in Digestive Endoscopy Experience of Managing the Intake of Button Batteries in the Digestive Tract in Infants". Acta Scientific Gastrointestinal Disorders 7.10 (2024):08-12.
The ingestion of a button battery is an emerging problem due to the lesions it can cause on the mucosa of the digestive tract. Children under 6 years of age are a high-risk group. X-ray imaging was essential for the identification and location of the batteries. Extraction should be performed by endoscopy in the shortest possible time, before burn injuries, perforations and strictures occur.
We documented our experience of 17 cases of ingestion of button batteries in the digestive tract. Removal of the batteries by endoscopy was performed in 15 cases. One case required a laparotomy due to perforation of the small intestine, in another case it was allowed to be expelled along with the feces. Mucosal lesions were observed in 4 infants, associated with a longer contact time of the piles with the digestive mucosa.
A prevention campaign should be carried out by specialized medical societies, to avoid these accidents in homes, as well as to raise awareness among pediatricians and gastroenterologists of the risks of a delay in diagnosis and extraction.
Keywords: Button Batteries; Esophageal Burn; Dysphagia
Swallowing a foreign body (FB) usually occurs in children inadvertently. The most frequent age is 6 years old, especially in boys and accidentally, either due to carelessness or curiosity to put everything in their hands in their mouths. Complications are very low and mortality is almost zero [1]. Among the variety of ingested objects we find coins, buttons and safety pins, small toys, pencils, puzzle pieces. The ingestion of flat coin or button batteries by infants has gained great interest in recent years due to an increase in their frequency and the high risk of morbidity [2], constituting a serious emerging problem.
These PBs are not rechargeable and although relatively small, they have a very long average life of useful use. They are used in toys, car keys, watches and in multiple objects of daily use in the home [3].
The chemical composition and its electrical voltage provide the ideal conditions for damage to the digestive mucosa and a risk of systemic toxicity. Batteries are generally made up of 4 main components, Mercury Oxide, Silver Oxide, Manganese Oxide and Lithium Oxide, all dissolved in a solution of 20-45% Potassium or Sodium hydroxide. This chemical combination favors an oxidation-reduction reaction, which determines an electrical voltage of 1.5 to 3.6 volts, depending on the model and size.
From contact with the digestive mucosa, a low-voltage electrical burn begins, then the degradation of the metal structure of the battery casing and the exit of its alkaline content occurs, producing direct chemical lesions due to corrosion and necrosis of the mucosa [4-6].
Within an hour, erythema, congestion, and necrosis may be observed. A perforation of the wall of the digestive tract is observed within 4 hours. Finally, these lesions can evolve to the formation of tracheoesophageal, entero-enteral fistulas and a stenosis could be constituted between 3 to 14 days. Although mortality is low, the delay in diagnosis is a factor in the occurrence of complications and the triggering of eventual fatal injuries [7].

Figure 1
Intestinal perforation secondary to a button cell swallowed 20 hours earlier in a 7-year-old boy. Own source.
Normally, there are no initial signs of choking or dysphagia with PBs, whose diameter does not exceed 11.6 mm. On the other hand, larger PBs (24.5 mm) can cause dysphagia, especially in young children. Later, retrosternal pain, burning sensation, and dysphagia may occur. In infants, incessant crying, odynophagia and refusal of food are frequent and should lead to suspicion of an EC in the esophagus. In older infants, the same interrogation reveals dysphagia and may make us suspect the type of EC ingested.
The anamnesis must take into account the approximate time of intake of the battery, feeding schedules, medications, as well as a complete medical history of the patient.
Anteroposterior and lateral radiographs of the chest and abdomen determine the presence of a flattened round object, opaque radius, with characteristics similar to a coin. The typical concentric opaque radius halo allows us to affirm that it is a battery, in addition to its size and location.
The extraction of a BB located in the upper digestive tract must be performed urgently, in the safest conditions for the patient, either in the operating room or in an endoscopy unit with the possibility of offering general anesthesia with endotracheal intubation assisted by an anesthesiologist. All this to protect the airways and prevent a possible passage of the BB into the trachea, as well as offering the greatest safety to introduce and manipulate the endoscope inside the digestive structures of small diameter.
PBs located in the esophagus should be removed immediately by endoscopy. If the infant is younger than 5 years of age and the battery measures 20 mm or more, immediate removal by endoscopy is recommended [8,9].
The most distal batteries in the digestive tract should be within reach of the endoscope and removed immediately, using mouse-bite forceps or with a polyp basket. If they have progressed to the small intestine and there are no signs of perforation, patients are observed on an outpatient basis, using a laxative to speed up their transit and allow their recovery in the stool. If it is not expelled within 24 hours, or if symptoms develop, we should repeat the images and consider endoscopic extraction.
After extraction, if there was mucosal damage, it is necessary to leave the patient hospitalized, under observation and under treatment, for at least 24 hours until a complication is ruled out and the oral route can be reestablished. A liquid diet based on honey has recently been proposed with the aim of mitigating tissue injury pending possible definitive treatment. Animal studies have shown benefit and a reduction in the extent of lesions [10-12].
The ingestion of a BB is an event that occurs more and more frequently in pediatric emergencies. There is potential damage to the digestive mucosa, especially associated with the size of the BB and the time it remains attached to the mucosa before its removal.
After diagnosis and location by imaging, an urgent endoscopic extraction should be performed. Mouse bite tweezers or baskets are the most suitable instruments. Mucosal damage should be observed and treatment with cytoprotectants, proton pump inhibitors, liquid diet, and close observation should be initiated.
An awareness campaign among the general population about the correct final disposal of PBs and any object with toxic content and thus avoid these accidents in homes. Pediatricians, emergency physicians, and gastroenterologists should be aware that delay in the diagnosis and removal of a BB can be associated with significant mucosal lesions, with eventual permanent sequelae.
We would like to report our experience in the cases of management of the intake of flat button batteries (BB) by infants, who were assisted in the Pediatric Emergency and then referred to the Digestive Endoscopy Unit of the Center for Gynecology and Obstetrics of the City of Santo Domingo.
A retrospective study was carried out from January 2015 to August 2023, the records of all cases of ingestion of foreign bodies in children were reviewed, selecting those who had ingested BB, finally a total of 17 patients were included.
Each file was reviewed, collecting general data, such as age, sex, time of ingestion of the battery, location in the digestive tract, mucosal damage, complications during the procedure and informed consent signed by the parents. Incomplete files were discarded.
In the review of the file, emphasis was placed on establishing precisely the time of intake of the EC, arrival at the emergency room and finally the start of the endoscopic procedure.
Classification of mucosal lesions.
The lesions on the mucosa were classified as mild: presence of a mucosa with well-defined erythema, without loss of epithelial continuity. Moderate: we observed a depressed mucosal lesion, with a fibrinoid background, ulcerated, with a halo of erythema and edema around it. Severe: circumferential burn, very depressed, necrotic, blackish, with significant loss of the mucous layer, eventually hemorrhages.
An informed consent was signed by the parents or guardians of the patients before the intervention, explaining the extraction procedure, the available alternatives, indications, contraindications, consequences and results, both of the extraction procedure and of the anesthesia. In addition to authorizing the use of the information regarding the case for scientific dissemination, respecting the identity of the patient.
17 infants aged from 16 months to 7 years were assisted, of which 11 were males and 7 females. Most of the PBs were located by X-rays, in the esophagus (12), the stomach (3), in the small intestine (1) and in the colon (1).
The time elapsed between the time when ingestion was suspected and arrival at the emergency room was on average 163 minutes (40 to 360 min). Then, from the initial evaluation by the pediatric emergency service, the radiological diagnosis and finally the implementation of the endoscopic extraction procedure, the time elapsed was no more than 120 min.
Of the total of 17 cases, 15 were successfully extracted endoscopically. One case by laparotomy and one case was allowed to leak in the stool.
All endoscopic extraction procedures were performed in the operating room under endotracheal intubation, with the assistance of a trained anesthesiologist. No problems related to anesthesia were reported.
After the extraction procedure and recovery from the effects of the anesthetics, an alkaline liquid diet associated with topical cytoprotectants such as sucralfate, magaldrate-simethicone, as well as milk, was initiated in 11 cases. In patients with the most significant mucosal burns, a few hours were waited, starting the oral route only with cytoprotectants. We have recently included the use of honey in the diet of patients with significant burns of the esophagus.
In one case, removal by the surgical team was necessary. It was a 7-year-old male who presented acute abdominal pain, associated with signs of peritoneal irritation. The physical examination revealed an acute abdomen. In the clinical history, the patient reports having ingested the BB approximately 20 hours before.
Radiological images showed a small round image, of metallic density suggestive of a BB, located in the center of the abdomen, presumably in the small intestine, in addition to radiological signs of subdiaphragmatic air. Under the diagnosis of hollow viscera perforation, an open laparotomy was performed with the finding of a button type battery perforating the wall of a thin loop, an external suture was performed to repair the defect. The clinical evolution was satisfactory, without complications and he was discharged 4 days later.
A second case, located in the large intestine, did not require any extraction procedure. It was a 6-year-old female, who accidentally ingested the BB along with food, 130 minutes before being assisted in the emergency room, so at the time of diagnosis it was located in the transverse colon. The decision was made to let progress until his expulsion by normal routes helped by laxatives, which occurred without incident.

Figure 2
Radiological image of a 6-year-old female showing BB located in the transverse colon. Own source.
In the cases reviewed, there was no mortality.
The most serious complications occurred in 4 patients, 3 males and 1 female, aged between 1.8 and 4 years. These patients had an average of 270 minutes between ingestion and arrival at the emergency room (180-300 min), with endoscopic findings of major burns in the middle esophagus and gastric antrum evidenced during endoscopy.
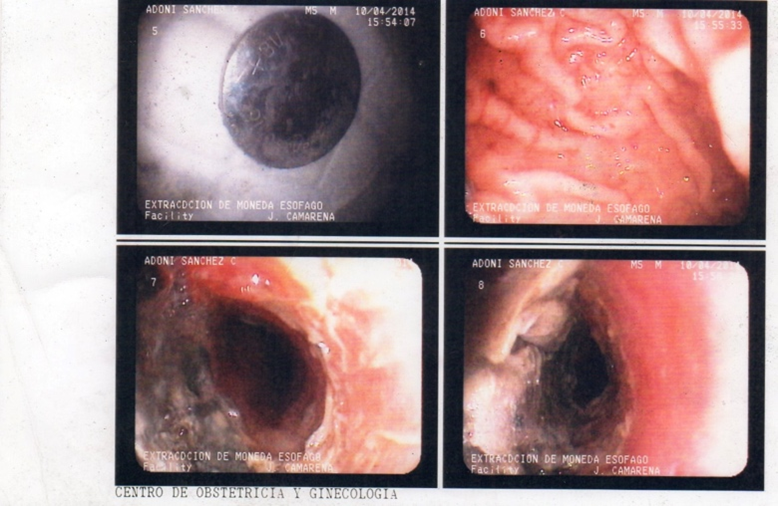
Figure 3
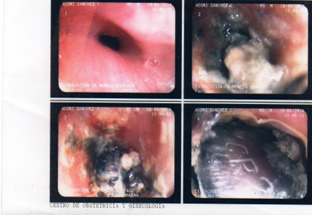
Figure 4
The most important lesions in the esophagus and stomach were associated with larger BB and a time spent in contact with the mucosa of more than 4 hours.
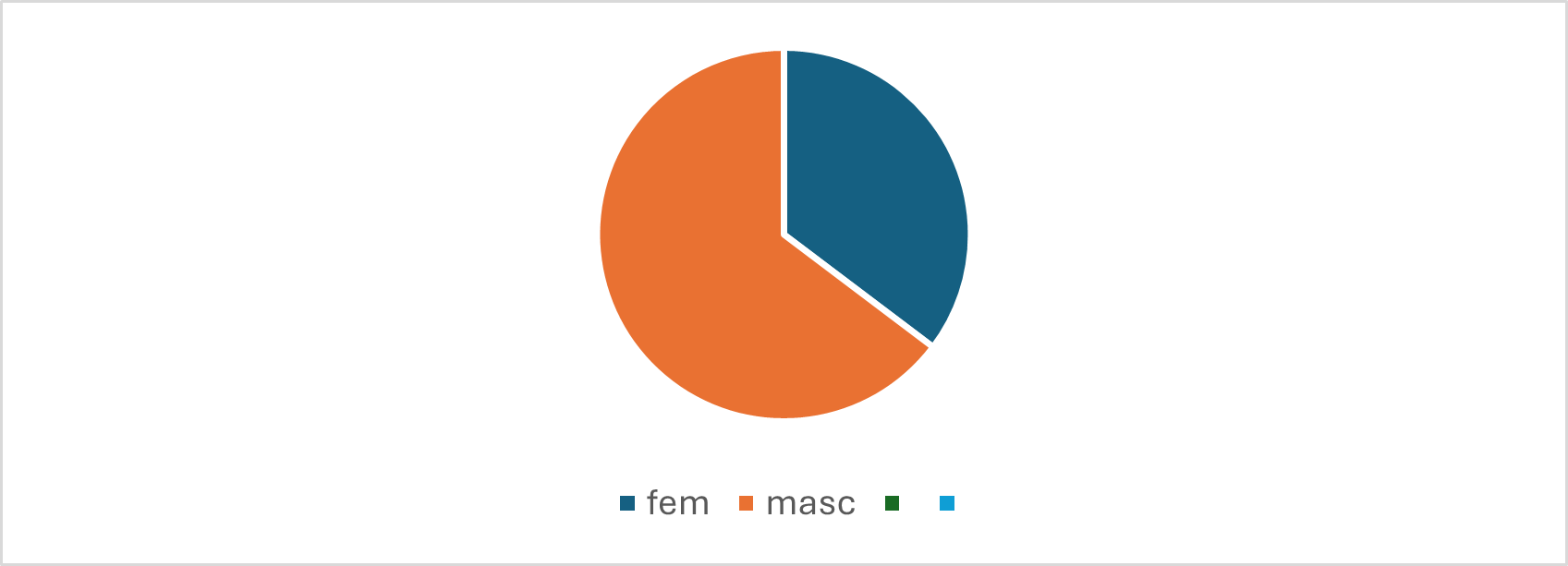
Figure 5
Distribution of cases of ingestion of button batteries in the upper gastrointestinal tract in the period 2017-2023, in the endoscopy unit of the Obstetrics and Gynecology Center, Santo Domingo, Dominican Republic.
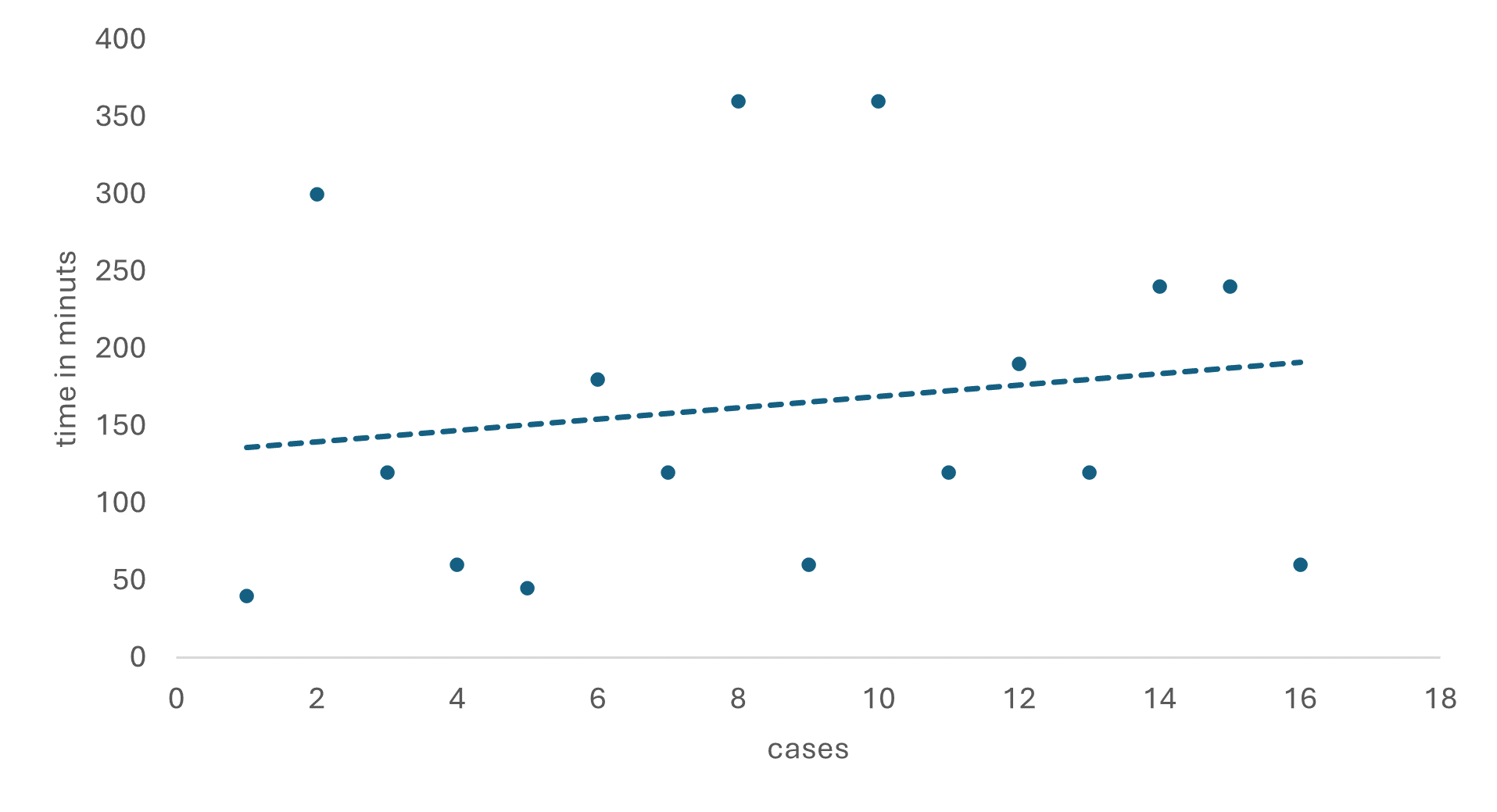
Figure 6
Estimated time in minutes between the time of ingestion and arrival at the emergency room of patients who ingested button batteries, in the Endoscopy Unit of the Center for Gynecology and Obstetrics, Santo Domingo, Dominican Republic.
A review of 17 cases of type BB CE was performed in the Endoscopy Unit of the Obstetrics and Gynecology Center of the City of Santo Domingo. Most were male, aged from 16 months to 7 years, of these 15 cases were resolved by extraction by digestive endoscopy, one case by laparotomy due to a perforation of the hollow viscera and one case was allowed to be expelled in the feces.
The average time between intake and extraction was 163 minutes. The time elapsed between admission to the emergency room, diagnosis, and endoscopic extraction was no more than 120 min.
The deleterious effect of the toxic content of PBs was associated with a larger size of the PBs and more time in contact with the mucosa. These patients manifested greater symptoms of esophageal dysphagia and more severe lesions in the esophagogastric mucosa were observed.
We believe that a rapid endoscopic intervention, after diagnosis, is appropriate to achieve a reduction in mucosal lesions and sequelae. Agility in triage in the emergency room, as well as prompt and formal referral to the Endoscopy Unit are the key elements to reduce acute injuries and possible long-term sequelae.
Copyright: © 2024 Camarena J., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff







