Akpe JO1, Nwoga MC2, Ogbozor BC3 and Chukwuneke FN4*
1Senior Lecturer/Consultant ENT Surgeon, College of Medicine, University of Nigeria
Ituku-Ozalla Campus, Nigeria
2Senior Lecturer/Consultant Oral Pathologist, College of Medicine, University of Nigeria
Ituku-Ozalla Campus, Nigeria
3Lecturer 11/Senior Resident Surgeon, College of Medicine, University of Nigeria Ituku-Ozalla Campus, Nigeria
4Professor/Consultant Oral and Maxillofacial Surgeon, College of Medicine, University of Nigeria Ituku-Ozalla Campus, Nigeria
*Corresponding Author: Chukwuneke FN, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, College of Medicine, University of Nigeria Ituku-Ozalla Campus, Nigeria.
Received: June 03, 2024; Published: September 20, 2024
Citation: Chukwuneke FN., et al. “A 10-Year Clinical Evaluation of Maxillofacial Trauma Admissions in Enugu Southeast Nigeria". Acta Scientific Dental Sciences 8.10 (2024):41-46.
Introduction: Trauma-related injuries are a major cause of concern worldwide and constitute a serious public health issue in the developing world as well as in the developed countries. In Nigeria, the situation is worst because of many factors such as socioeconomic, bad roads and method of transportation, poor rescue operation, increasing violence, lack of hospitals with good facilities for resuscitation and early management of accidents victims.
Objectives: This study aims to evaluate the cause and potential risks associated with Maxillofacial trauma which can help to formulate future safety planning program for implementation of preventive measures in management of maxillofacial trauma patients.
Patients and Methods: Case notes of all the admitted maxillofacial trauma patients were retrieved, examined and analyzed. Data collected includes socio-demographic data, diagnosis, duration of hospitalization and treatment outcome. The pattern, distribution and treatment outcome of the injuries were evaluated.
Results: A total of 126 cases were analyzed out of which the major indication for admission were road traffic accident (RTA) 83 (65.8%), Gunshot injuries 15 (11.9%), Assaults/Fights 10 (7.9%), Domestic violence 5 (4%), Domestic accidents 4 (3.2%), fall from height 4 (3.2%), Sports 3 (2.4%) and Occupational accidents 2 (1.6%). In all there were 82 (65%) males and 44 (35%) females’ patients given a male-to-female ratio of approximately 2:1. Amongst the 82 male patients 8 (9.7%) were discharged without treatment against doctor’s advice and these included 3 cases of gunshot injuries and 5 maxillofacial fractures.
Conclusion: Road traffic accident had the highest proportion of the entire maxillofacial trauma followed by gunshot injuries which calls for a reinforcement of measures for the prevention of automobile accident and the increasing rate of violence in our society.
Keywords: Maxillofacial Trauma; Pattern and Distribution; Management; Treatment Outcome
In the specialty of oral and maxillofacial surgery, trauma injuries constitute a major problem especially in the developing world [1]. Trauma-related injuries are a major cause of concern to many clinicians worldwide and the rate of occurrence is on the increase [2]. Road traffic accidents by far constitute the major part of cases of maxillofacial facial trauma seen in our unit. Studies by several authors have implicated road traffic accidents as the major cause of traumatic injuries [3-5]. Any part of the body can be affected but the commonest causes of fatality are the head and neck injuries [6,7]. With the rise of violence in the society, maxillofacial injuries due to violence is on the high side. The extreme of age is affected, probably due to the fact that they are less active and most of the times indoors [7,8] Trauma injuries generally are public health issues in the developing world today and even in the developed countries. In all industrialized countries trauma injuries are the major cause of death and morbidity among all ages. In our environment Nigeria, the situation is worst because of many factors such as socioeconomic, bad roads, method of transportation, poor rescue operation, increasing violence in the society, lack of hospitals with good facilities for resuscitation and early management of accidents victims to mention but few [9,10]. The rate of maxillofacial injuries occurring in our environment is alarming and the situation has not been favourable to proper patients’ management [11]. This is because most of the times, these injuries result in prolong stay in the hospital as a result of lack of theatre space or patient’s inability to provide the necessary operation materials that the hospital do not have. In some cases, multiple surgical procedures and rehabilitation are required thereby denying new patients the chances of using the limited hospital facilities [12]. The high cost of treatment and long leave of absence from work place has a great impact on the income of the victim, his or her family and the country as whole. In some cases, the disabilities resulting from the trauma could cause both physical and psychological handicap to the patient which may lead to road side begging especially where the patient could not afford the cost of his or her treatment. The fact that these aetiological factors and causes of maxillofacial trauma are modifiable risk factors emphasizes the need for increasing awareness among the general public and policy makers as a first step in the prevention of occurrence of this accidental disorder.
We carried out a 10-year retrospective evaluation of 126 cases of maxillofacial trauma admission in three specialist hospital in Enugu, Nigeria between January 2011 and December 2020. The study took place at the Oral and Maxillofacial Surgery units of the University of Nigeria Teaching Hospital (UNTH) Enugu, Godfrey Okoye University Teaching Hospital Trans-Ekulu, St Leo Specialist Hospital Trans Ekulu all in Enugu, south eastern Nigeria. These patients were referred to the unit by the dental surgeons, medical practitioners and health centers in the catchments area of the hospital because maxillofacial injuries were involved. The catchments areas are the south-eastern states, the Delta state and the Benue state of the Federal Republic of Nigeria. We retrieved the case notes of these patients from the records department, analyzed and evaluated. Relevant information about the patients’ collected include; socio-demographic data, diagnosis, duration of hospitalization and treatment method. The pattern, distribution and treatment outcome of the injuries were equally evaluated. Clinical and laboratory findings at the time of admission were noted. To study the pattern and trends in the yearly occurrence, we grouped the cases by the year of presentation and the site of distribution and diagnosis. Data collected were evaluated, analyzed and converted to relative value for generation of statistic. We analyzed and processed the data collected using the analysis of variance (ANOVA) technique and chi-square (χ2) test of comparison on the etiology and the injury distribution with STATA statistical software. The level of significance was set at 0.05 where p < 0.05 is considered significance and p > 0.05 non-significant.
Out of the total of 126 oral and maxillofacial trauma cases admitted in the department of oral and maxillofacial surgery of the three specialist hospitals, 82 (65%) were males and 44 (35%) females given a male-to-female ratio of approximately 2:1. The major indication for admission and pattern of trauma distribution were road traffic accident (RTA) which accounted for 83 (65.8%) while Gunshot injuries cases ranked second 15 (11.9%) in line of sequence. Others in descending sequence were, Assaults/Fights 10 (7.9%), Domestic violence 5 (4%), Domestic accidents 4 (3.2%), Falls 4 (3.2%), Sports 3 (2.4%) and Industrial accident 2 (1.6%). The age range of the patients were between 7-74 years with mean age of 34 years (SD + 6.4). Analysis of the aetiology of the injuries sustained from RTA (83; 65.8%) showed that motorcycle accident popularly known as Okada in Nigeria was responsible for 65 (79.3%), and 18 (20.7%) were due to motor accident (Table 1). Of the 15 (11.9%) cases of gunshot injuries, 11 (73.3%) were sustained from low velocity missile while 4 (26.7%) by high velocity missile. Information on the data recorded showed that violence was responsible for 13 (89%) cases and 2 (11%) were due to the accidental discharge (Table 2). Most of the gun shot injury patients were between the ages of 21-40 years (72.5%). All the patients had various degrees of hard and soft tissue injuries. Injuries from Assualts/Fights were common among the age group of 16 to 39 years with 6 (60%) out of the 10 cases recorded sustaining mandibular body fracture, 2 (20%) had Parasymphyseal and the rest 2 (20%) displaced zygomatic arch fracture. Domestic violence accounted for 5 (4%) of which wife bettering with mandibular fracture was 4 (80%) while facial laceration and stab injury case admitted was one person (20%.). Almost all the admissions on domestic injuries were females 80% while 20% was a male with the laceration and stab injuries. All the female patients with domestic injuries were blunt trauma with resultant fractures or severe contusion necessitating hospitalization. Overall, the highest recorded number of maxillofacial admissions was in 2010 while the lowest was in 2016 (Figure 1). Amongst the 82 male patients 8 were discharged without treatment against doctor’s advice and these included 3 cases of gunshot injuries and 5 maxillofacial fractures. For those gunshot injuries with low velocity missiles, management method was conservative. Patients with mandibular fractures were treated with reduction and immobilization using arch bars and 0.5 stainless steel wires depending on the type fracture sustained (Figure 2) while for some, bone plate rigid fixation were employed (Figure 3).
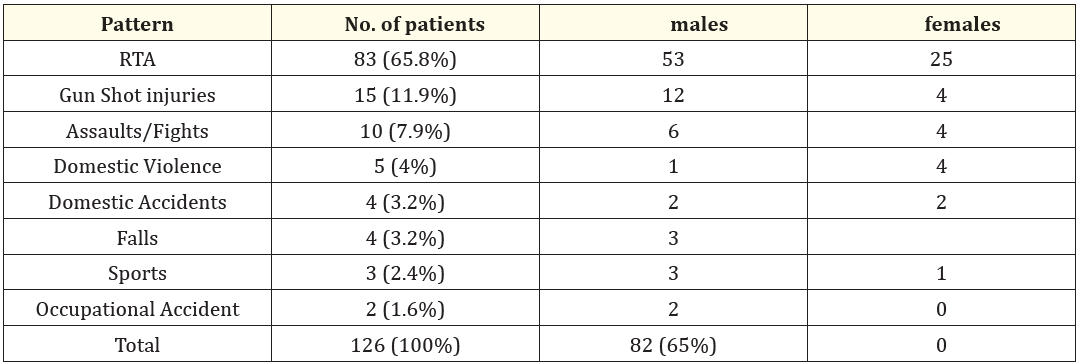
Table 1: Pattern of distribution of Maxillofacial Trauma adjusted by the sex.

Table 2: Comparison of etiology of RTA and Gunshot injuries with Chi square test of significant.
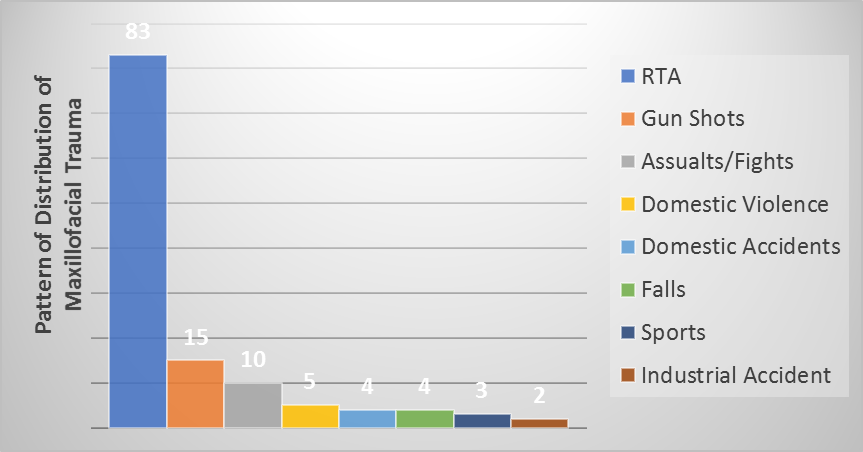
Figure 1: Major indication for Admission and pattern of Trauma Distribution
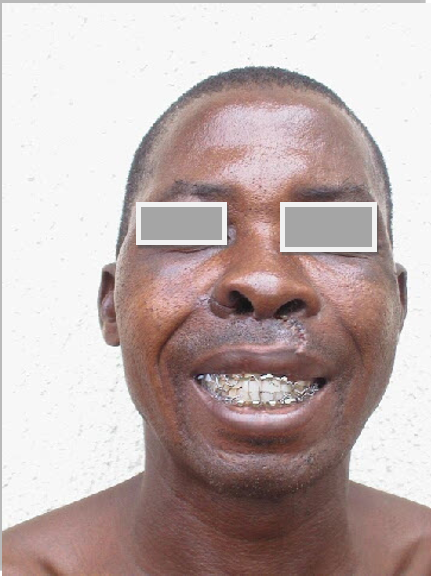
Figure 2: Patient after mandibulo-maxillary fixation with arch bars.
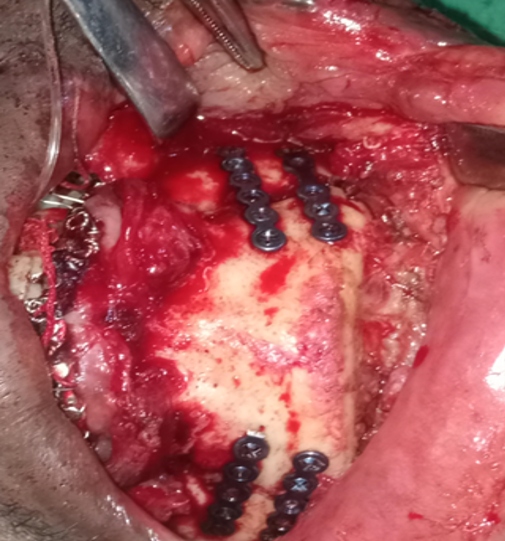
Figure 3: Bone plate rigid fixation.
Maxillofacial trauma injuries and pattern of distributions have been severally documented in literature by various authors [13-18]. Several studies worldwide on the etiology of maxillofacial injuries shows that incidence varies from one country to another and even within the same country depending on the prevailing socioeconomic, cultural and environmental factors [19,20,21]. Some authors [22] have observed that Sports-related trauma tends to occur more frequently in higher socioeconomic areas, while Brasileiro., et al. [23] reported a high incidence of violence- related trauma in lower socioeconomic strata. A number of studies indicate substance abuse to be a major contributing factor to the occurrence of facial injuries within the variable of interpersonal violence [24]. A study by Desai., et al, conducted in South Africa reported that 65% of their cases of maxillofacial trauma were associated with alcohol [25]. This suggests that there is a significant correlation between alcohol consumption, interpersonal violence and maxillofacial trauma in their environment as different geographical areas also demonstrate different patterns of cause and presentation [26]. In Nigeria, studies in the different geographical areas indicate that the incidence of maxillofacial fractures from trauma have been on the increase over the years [13,15,26]. Literature reviews have shown that road traffic crashes remain the major cause of maxillofacial injuries in Nigeria, unlike in most developed countries where assaults/interpersonal violence has replaced road traffic crashes as the major cause of the injuries [19]. In our study, we observed that of the 126 maxillofacial trauma cases admitted, 83 (65.9%) were due to road traffic accident of which 65 (79.3%) were due to motorcycle properly called Okada. Therefore, periodic auditing of the etiology and pattern of maxillofacial injuries should be given priority in our health policy which will help in assessing the proficiency of road safety measures such as speed limit, drunk driving, and seat belt laws as well as the individual behavioral patterns and mental fitness to handle automobile. The highest maxillofacial admission due to road traffic accident was in 2013 with 16 cases (19.3%) recorded. On the other hand, violence seems to be on the increase as our study recorded the gun shot injuries as the second highest occurrence within the study period. The year 2011 witnessed the highest rate of guns shot injuries 4 (26.7%) followed by 2015 with 3 (20%) for the 10-year evaluation period. This may be as a result of the violence that often characterize the election period which incidentally was in the year 2011 and 2015 respectively. Notwithstanding, the rate of violent activities cannot be compared to what is obtainable in other part of the country [12, 26] because of the serenity and peaceful nature of Enugu city. Since evidence suggests that etiology, incidence and patterns of maxillofacial and associated injuries vary with geographic location as well as the socioeconomic status of a population therefore, epidemiological data are central and should be taken into account while developing strategies to improve healthcare in a given population [28]. Most of the patient treated had good treatment outcome with 2 weeks median stay in the hospital from the time of admission to the discharge. However, eight patients (6.3%) were discharged without treatment against doctor’s advice and these included 2 cases of assault/fights injuries, a case of domestic violence and 5 fractures cases.
Road traffic accidents followed by gunshot injuries were the main cause of the maxillofacial injuries with more males affected than females. The fact that these aetiological factors and causes of maxillofacial trauma injuries are modifiable risk factors emphasizes the need for increasing awareness among the general public and policy makers as a first step in the preventive measure. In the same light more maxillofacial specialist centers should be established to help administer treatment to the patients as early as possible.
Copyright: © 2024 Chukwuneke FN.,et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff








ff
© 2024 Acta Scientific, All rights reserved.