Gurkeerat Singh, Harshita Gupta, Anu Rathi*, Deepali Bisht, Varun Goyal, Raj Kumar Singh and Sonali Dhawan
Department of Orthodontics and Dentofacial Orthopaedics, Sudha Rustagi College of Dental Sciences and Research, Faridabad, Haryana, India
*Corresponding Author: Anu Rathi, Postgraduate Resident, Department of Orthodontics and Dentofacial Orthopaedics, Sudha Rustagi College of Dental Sciences and Research, Faridabad, Haryana, India.
Received: March 01, 2021; Published: : March 29, 2021
Citation: Anu Rathi., et al. “The Use of Bite Raisers in Orthodontic Treatment - A Review of Literature”. Acta Scientific Dental Sciences 5.4 (2021): 219-228.
Patients undergoing orthodontic treatment often require temporary bite raisers primarily for disocclusion of the dentition and unobstructed tooth movement. Depending upon the type of malocclusion and the desired treatment result, a variety of bite raisers can be fabricated. They improve dental and facial balance as well as gives relief from temporomandibular joint disorders (TMD) symptoms. This article reviews the different bite raisers currently used in day-to-day practice along with their biomechanics involved and in deciding their position, duration, thickness and material used.
Keywords: Bite Raiser; Vertical Dimension; Orthodontics; Openbite; Crossbite; Scissorbite; Occlusion
CR-CO: Centric Relation-Centric Occlusion; GIC: Glass Ionomer Cement; TMD: Temporomandibular Joint Disorders; ABPFA: Anterior Bite Plane Functional Appliance; NTI-tss: Nociceptive Trigeminal Inhibition Tension Suppression System; RMI: Rapid Molar Intruder
Bite raising is a fairly old and commonly practiced concept in the field of orthodontics. A bite plane is an artificial surface especially fabricated either anteriorly or posteriorly to provide a plane against which the teeth of the opposing arch can contact when brought together for occlusion such that full closure of the jaws is prevented. The bite is thus said to be raised. The orthodontic correction of deepbite, openbite, scissorbite and crossbite often requires temporary bite opening which serves to eliminate occlusal interferences, improve CR-CO (centric relation-centric occlusion) discrepancy, provide unhindered tooth movement by preventing unwanted breakages of the orthodontic brackets [1-3].
The first inclined plane was described by John Hunter in 1771 which was fabricated on the lower anterior teeth to correct a lingually blocked out tooth. Henry Clay Quinby and W.G. Bonwill later on described the maxillary bite plate for deepbite correction and N.W. Kingsley introduced the maxillary bite plate to jump the bite [4]. These appliances help to disarticulate the posterior teeth; deprogram the masticatory muscles; and allow for eruption, extrusion, and uprighting of the posterior teeth [5].
In the original designs, the bite plates were constructed to fit the patient's palate. As time went by, to meet patient comfort and compliance, they evolved to have a more compact and convenient form which were easily attached to the teeth. These are most commonly used orthodontic auxiliary and are often described as 'bite plates', 'bite planes', 'bite blocks', 'bite raisers', ‘bite ramps’, ‘occlusal build ups’, ‘disarticulators’ and 'bite turbos'. They can be removable or fixed [6-9] and can be placed in the anterior or posterior segment of the mouth with respect to either maxillary or mandibular arches depending on the individual treatment need (Figure 1). Removable bite plates though convenient depend largely on patient cooperation and require frequent adjustments to account for orthodontic tooth movements. They can easily be lost or broken and sometimes swallowed by the patient as well [10]. They may also lead to the creation of plaque accumulation areas resulting in poor oral hygiene and high risk of dental caries [11,12]. Gagging due to over-extended bite plates and ulcers in the oral cavity due to sharp ends are amongst the common problems caused by the removable plates. Banded bite plates provide a fixed alternative, but they are less accommodating of tooth movements and can cause soft-tissue irritation. Other fixed bite turbos can be either fabricated with glass ionomer cement (GIC) or composite resin; or metal fixed bite raisers can be utilised as described by Joe Mayes in 1994 [13]. Fixed bite-turbos are hygienic, minimizes bulkiness, reduce interference with speech and is less intrusive on the tongue space when compared to the conventional acrylic plates [1].

Figure 1: Classification of bite planes.
Bite planes have thus traditionally been used to correct a variety of malocclusions and results have not only shown improvement in dental and facial balance but also relief of various TMD symptoms. However, whether the problem in the joint is cured or not is a matter of much debate and beyond the scope of this review. Over the years a number of bite planes have been developed in response to different treatment needs and this article aims to review those that are currently used in practice.
Indications of disarticulationAn anterior bite plane is generally given when disocclusion and changes in posterior dentition are required; in deep bite cases that are a result of infraeruption of posterior teeth and decreased lower facial height or when disengagement of posterior contact is required to correct posterior crossbite and maxillary expansion.
Hawley anterior bite plateit is a removable bite plate and is a regular Hawley appliance with an added acrylic platform in the anterior region behind upper incisor teeth which is made parallel to the occlusal plane (Figure 2). The lower incisor bites on this plane leaving a gap between the posterior teeth. This warrants the elongation of posterior teeth which depends on the growth of alveolar bone. The new bone needs to be conditioned to withstand the stresses of mastication by the withdrawal of the bite plate gradually. These bite plane basically causes a differential eruption of posterior teeth causing reduction of deep bite and also cause relative intrusion of anterior teeth (by causing proclination) leading to levelling of curve of spee. Further, in the case of posterior dental crossbite, the disocclusion of teeth enables easy use of cross elastics for correction. Moreover, in many cases of temporomandibular disorders, relief of pain, clicking and other symptoms of joint have been reported after the use of this plane. This was accredited to unloading of joint, relaxation of lateral pterygoid muscle and other elevators and neuromuscular deprogramming are among other reasons [11].

Figure 2: Hawleys anterior bite plane.
The height of anterior bite plane should not interfere with freeway space and there should be a clearance of 2 - 3 mm space in posteriors. Patients might place their tongue in the gap between posteriors if it is of more than 3 mm thus hindering the teeth from freely erupting. At the same time, high anterior bite planes may cause undue pain and trauma to the masticatory muscles, TMJ and lower incisors. This may also cause unfavourable clockwise rotation of the mandible, which may not be desired. It is desired that anterior bite plane may be gradually raised as clinician monitors the bite opening in progress. Along with height, inclination of plane is also an important factor to reduce the undesired effects. A bite plane should be vertical to the long axis of lower incisors so as to generate forces parallel to the long axis and therefore causes intrusion of the incisors [11]. This careful consideration regarding height of bite planes is applied to all its modifications as discussed in the succeeding literature.
Sved bite planeIn 1944 another type of bite plane was introduced to reduce the side effect of proclination by the name of Sved bite plane, in this acrylic plate was extended up to the incisal edge of upper anteriors which prevented forward component of force and thus reducing proclination of anteriors [11,15].
Bite plate with expansion screwThe use of a removable appliance with a jackscrew and anterior bite plate was shown to be beneficial in the correction of deep bite for those with transverse deficiency in mixed dentition stage [11,15].
Bite plate with reverse inclined planeIt looks like a flat anterior bite plane, the difference is the incorporation of the anterior incline plane to engage lower incisors and cause the mandible to slide anteriorly. The appliance with a reverse incline is useful in growing children with a mild superior protrusion, deep bite and mandibular retrusion. It is also used as a retention appliance after active functional therapy like twin block [16]. The upper anterior incline plane favors the forward movement of mandibular teeth from distal occlusion into neutral occlusion. To ‘lock’ the lower incisors in a desired forward position of the mandible, incisal edge indentations of lower incisors can be incorporated in the bite plane. This technique needs good vigilation of the occlusion by the clinician as it leads to the flaring of lower incisors [11].
Catalan’s applianceIt was introduced 150 years ago. In Catalan’s appliance (Figure 3), lower inclines are used to correct the anterior crossbite. It causes the opening of a bite by the eruption of posterior teeth. It is used during the eruptive stages of incisors. The incline of 45 degrees guides the lingually erupting incisor into proper occlusion. It is worn a maximum of 3 weeks but if it is worn for a long time it leads to anterior open bite due to over-eruption of posterior teeth [17].

Figure 3: Catalan’s appliance.
The NTI-tss is a prefabricated anterior bite block that caps the maxillary or mandibular incisors. It has been used to provide relief in cases of bruxism, temporomandibular disorders (TMDs), and migraines [18]. The NTI is customized for proper fit with the help of acrylic or thermoplastic material which is added into the base of the device and adapted along with the teeth. The NTI is adjusted such that no contact occurs between the posterior teeth during mandibular movements. It is meant to be used at night, but variations are available for wear during the daytime as well.
Anterior bite turbos Metal turbosIn 1994 Joe Mayes of Ormco Corporation created metal bite turbos [13]. It was a simple modification of a lingual upper incisor bracket. Mayes believed metal was a better material for deprogramming the muscles than the soft acrylic used in conventional bite planes. It was simple, durable and there was the ease of fabrication. But sometimes it was difficult to place because of the variability of upper incisor lingual anatomy and also there were lisping and Intolerable tooth vibrations [10].
Resin turbosBecause of the shortcomings with metal turbos another type of turbos was introduced i.e. resin turbos. Different materials like acrylic gels, band cement, bracket adhesives, and lingual retainer adhesive can be used to make turbos. They can be fabricated chairside via direct or indirect method or may be 3D customized [10]. Anterior resin turbos are indicated in low-angle patients, though anterior turbos should be used with caution in high-angle cases because of the risk of undesirable posterior extrusion. The most common site for anterior resin turbos is on the lingual aspect of the upper central incisors. Both central incisors are bonded to distribute the occlusal forces. Upper lateral incisors are rarely used because of their shorter roots, although this could be an alternative location if the patient develops a lisp. The deeper the bite, the more incisal be the turbo fabrication. They should be long enough for lower arch not to slip behind it or move it gingival towards a thicker part of the tooth and to allow for more forward path of closure (Figure 4). To reduce the risk of fracture of long turbos, they can be placed on maxillary cuspids initially, then moved to central incisors as the overjet is reduced. However, this may cause the mandible slide sideways, condylar position will be asymmetric, and the patient will be prone to temporomandibular joint pain. Turbos are desired to be used for an average of 6 months, depending on how deep the initial overbite [10]. At the same time, the clinician need to be vigilant with regard to the periodontal health of the mandibular incisors as well.

Figure 4: Anterior resin turbos.
A modified version of the Nance appliance or palatal acrylic button is that which incorporates a bite plate [19] (Figure 5). This appliance is invaluable as a treatment accelerator, because it allows immediate placement of brackets on the lower anterior teeth. It can also maintain the vertical dimension in patients with early loss of primary teeth. In many TMJ cases, it is better than a removable splint because it frees the buccal occlusion from prematurities while allowing a natural path of lateral excursion.

Figure 5: Fixed anterior bite plate.
A posterior bite plane disoccludes anterior teeth for correction of anterior crossbite. They have also been used for correction of open bite, because of the vertical intrusive forces on the posterior segments. By intruding posterior teeth, along with correction of an anterior open bite, the mandible also rotates anticlockwise and thus decreases lower anterior facial height.
Hawley posterior bite planeIt is a removable posterior bite plane covering the occlusal surface of posterior teeth, hinging the mandible open by 3 - 4 mm approximately beyond its rest position. They have the advantage in applying essentially vertical forces, thereby causing decrease in the posterior dentoalveolar height, relative extrusion of anterior teeth and mandible rotates upward and forward [11]. This helps in correction of openbite. In cases of scissor bite, a ramp or inclined plane can be incorporated in the direction of desired tooth movement. Along with Z spring, it is used in crossbite correction in removable appliance therapy. Activated Z spring tips the tooth labially.
Posterior resin turbosPosterior resin turbos are indicated in average-angle cases. Posterior resin turbos are usually placed on the supporting cusps of the mandibular first molars [10] (Figure 6). They can be placed on mandibular second deciduous molars in preadolescent patients. Some clinicians prefer them to be placed on maxillary molars or premolars for the ease of fabrication as isolation is better. They can be extended over bracket pad for added bracket retention. According to Fiorelli and Melson [20], anchorage loss can be prevented by built-up composite onlay on mandibular posterior teeth, providing deep intercuspation.

Figure 6: Posterior resin turbos.
Bonded hyrax is often used for maxillary crossbite correction in hyperdivergent patients (Figure 7). Bonded posterior bite plane disoccludes posteriors for unhindered expansion and when kept for long intervals will result in intrusion of molars. For best results, the bite is raised 3 - 4 mm beyond freeway space. A unilateral cross-bite is often the outcome of convenient shift of the mandible due to bilateral maxillary constriction. A maxillary expansion appliance with posterior bite plane would disengage the mandible from its laterally locked position and enhance maxillary expansion. Posterior bite plane is also useful in bilateral posterior cross-bite with similar benefits [10].

Figure 7: Bonded posterior bite plane with expansion screw.
The spring-loaded block was described by Woodside and Linder-Aronson in 1986 [21]. These bite blocks cover the occlusal surface of posterior teeth and consist of helical springs made with 0.9 mm high strength stainless steel wires, the ends of which are embedded into the acrylic blocks. The helices are activated to deliver forces.
The bite blocks can be connected bilaterally with 1 mm ss wires or acrylic plates which can be extended up to the cingulum or can cap incisors to prevent their overeruption. They are activated from time to time, supplying additional force within the neuro-muscular system, besides the forces of the masticatory muscles. Because of its peculiar design, it was thought that the same appliance could also act as a habit-breaking appliance. With this appliance, the patient must apply active force to close his mouth, and this acts as a distraction therapy [22].
Rapid molar intruder (RMI)The rapid molar intruder was used by Carano to treat non-compliant patients with open bites. The device is fixed to the maxillary and mandibular molars with the help of bands. It consists of elastic modules and coil springs which help in the active intrusion of molars. On occlusion, a force of 800g is exerted on the teeth which is reduced to 450g by the end of the first week and 250g by the end of the second week. One drawback to treatment with RMI is buccal tipping of the crown as the line of action of the force is lateral to the center of resistance of molars. This can be counterbalanced by using transpalatal and lingual arches. The RMI can be modified to be used with bite blocks instead of molar bands. Tubes can be added to the buccal side of the blocks and the RMI inserted into it. This has the added advantage of distributing the force of RMI to the entire block instead of concentrating all the force solely on the molars [23,24].
Magnetic bite blocksDellinger was the first to use magnets for the correction of open bite. He called the appliance the active vertical corrector [25]. Repelling magnets are utilized in opposing arches to intrude teeth. Samarium cobalt magnets are used. Since this is a reactive material it needs to be sealed in the oral environment meant as saliva can act as an electrolyte. The magnets can be embedded in acrylic and used. This would prevent both corrosion and leakage of potentially harmful products. Later the MAD IV device was introduced in which neodymium iron boron magnets (three times stronger than samarium-cobalt magnets) coated with stainless steel were used. This appliance provide both lateral shearing forces and vertical forces.
Implant supported bite blocksThe intrusion of posterior teeth with the help of posterior bite blocks combined with skeletal anchorage is a relatively newer technique. The use of coil springs or elastics along with TADs compounds the effect of posterior bite blocks and allows for en-mass intrusion with good stability in non-growing patients. It however is a comparatively invasive technique requiring incisions for the placement of the implant. Buccal flaring is controlled with transpalatal arch. Hooks are incorporated into the acrylic blocks to facilitate easy application of the elastics [26].
Guray bite raiserThe guray bite raiser is a prefabricated temporary bite raiser. It is made to be inserted into the headgear tubes and then adapted over the occlusal surface of the molars. It is secured with ligature wire or elastomer and is available in two different sizes for children and adults. Its advantage lies in its ease of placement and less chairside time. No laboratory procedures are required [27,28].
Temporary bite raising crownsThese are crowns fabricated bilaterally on molars with self-cure acrylic and cemented onto teeth with GIC (Figure 8). Care must be taken to ensure proper occlusal contact bilaterally. They act as temporary bite raisers and help in the correction of anterior crossbite. They have the advantage of being less bulky and thus lesser speech impairment and are worn full time [29].

Figure 8: Temporary bite raising crowns.
When the turbos are beveled they are known as functional turbos. They are constructed with beveled occluding surfaces that guide the opposing teeth toward the desired positions. Their most common application is in the correction of a mild anterior crossbite [30]. Resin turbo material is bonded to the incisal edges of two or lower incisors and then beveled lingually. Upon contacting the beveled surface, the upper incisors are nudged forward and the lower jaw is directed posteriorly. The dental crossbite will usually be corrected in about three months (Figure 9a). They can also be placed on premolars to improve disarticulation in Class II patients. These turbos essentially operate like a bonded Twin Block appliance: the mandible is disarticulated and repositioned as the occluding premolars slide along the beveled surfaces (Figure 9b). The same technique can be applied in aligner patients by adding unfilled rectangular attachments to the occlusal surfaces of the aligners [10].

Figure 9a: Functional Turbos on mandibular incisors.

Figure 9b: Functional turbos for class II correction.
It helps the clinician to visualize the direction of expected tipping and plan the proper position, thickness and length of the bite plane. It should be noted that the following effects of bite raisers are only applied when fixed orthodontic treatment i.e. brackets or wire are not bonded to the teeth. As the mechanics of bite raisers differs when used with fixed orthodontic treatment and has been briefly explained in the scenarios above.
Effect of bite plane on incisor inclination when anterior bite blocks are placed in patient’s mouth (Figure 10)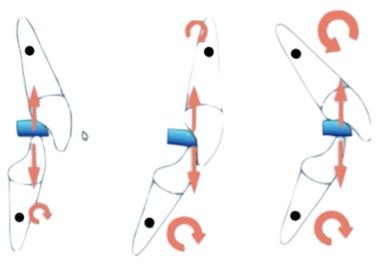
Figure 10: Effect of bite plane on incisor inclination.

Figure 11a: Effect of bite plane on molar inclination when molar is upright.
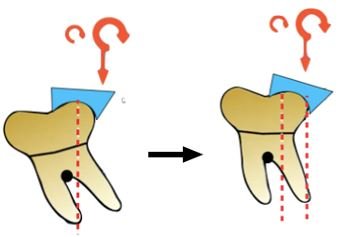
Figure 11b: Effect of bite plane on molar inclination when molar is mesially tipped.
Bite raisers are a valuable tool which helps in minimizing challenges of the orthodontic therapy. The position, thickness, and duration for which the bite plane is given is critical and determines treatment outcomes. A mandibular plane angle is also an important factor in choosing a turbo or bite plane location. The choice of bite raiser depends on facial type, amount of deepbite, skeletal relation and intended treatment mechanics. A good understanding of its action, method of fabrication and use is essential to avoid iatrogenic effects. Patient cooperation is variable and is not always forth coming, specially with removable bite raisers.
None.
Copyright: © 2021 Anu Rathi., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.









 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.