Lavanya Pasalkar*, Vikram Khare, Pallavi Channe and Shrutika Sonawane
Oral Medicine and Radiology, Dr. D.Y. Patil Vidyapeeth, Pune, India
*Corresponding Author: Lavanya Pasalkar, Oral Medicine and Radiology, Dr. D.Y. Patil Vidyapeeth, Pune, India.
Received: March 01, 2021; Published: March 24, 2021
Oral cancer is the most commonly seen malignancy in Indian males and leukoplakia is the commonest of all precancerous lesions which can transfer into oral carcinoma. The estimated global prevalence of oral leukoplakia is 2.60% with 0.13 to 34% malignant transformation rate. It has been proved that clinical type, grade of dysplasia and age are associated risk factors with malignant transformation. A 38 yrs male patient found to have a tiny solitary well defined white plaque like lesion on buccal mucosa hardly 2 mm x 3 mm which was unnoticed by the patient till then. Surface of the lesion was raised, rough and wrinkled. It was non-scrapable. Patient had tobacco and gutka chewing habit with cigarette smoking since 5 years. Though the size of lesion was too small considering all the factors provisional diagnosis of homogeneous leukoplakia was given. An immediate excisional biopsy was performed. Histopathological examination revealed oral leukoplakia with moderate dysplasia. Dysplastic changes could have been a major risk factor for malignant transformation. Early diagnosis and excision of lesion ensured good prognosis.
Keywords: Oral Leukoplakia; Malignant Transformation; Dysplasia; Premalignant
Oral leukoplakia is considered to be a premalignant lesion. A precancerous lesion is defined as a morphologically altered tissue in which cancer is more likely to occur than in its apparently normal counterpart [1].
Oral leukoplakia is one of the most commonly seen oral potentially malignant disorders in clinical practice. The estimated global prevalence of it is 2.60% with 0.13 to 34% Malignant transformation rate [2]. Because of multiple locations, often diffused margins and other associated risk factor for malignant transformation management of leukoplakia becomes difficult [3]. So early diagnosis and prompt treatment is beneficial. Here we have presented a case of tiny lesion of leukoplakia which could have been gone unnoticed and discussed importance of immediate treatment of same, with risk of malignant transformation.
A 38 years male patient reported to department of oral medicine and radiology for routine dental check-up. On intraoral examination a tiny solitary well defined white homogeneous plaque like lesion seen on left buccal mucosa which was till then unnoticed by patient. Lesion was hardly approximately 2 mm x 3 mm on buccal mucosa with respect to 34, 35. Surrounding mucosa showed hyperpigmentation (Figure 1). On palpation all inspector findings were confirmed. Surface of the lesion was raised, rough and wrinkled. It was non-scrapable and non-tender. No history of associated pain with same was given by patient. On asking habit history tobacco and gutka chewing habit since 5 years 8 - 10 times a day which he used to keep it in left buccal vestibule and habit of cigarette smoking 1 - 2 times a day since 5 years given by patient. Based on patient’s history and clinical examination provisional diagnosis of homogeneous leukoplakia was given. Patient was convinced for routine haematological investigation which reported to be within normal limit, patient made aware of his current diseased state and motivated for tobacco cessation.

Figure 1: Homogeneous leukoplakia on left buccal mucosa.
An excisional biopsy was planned and performed after taking written consent from the patient (Figure 2A):
Cotton rolls.
Excised tissue sent for histopathological examination with haematoxylin and Eosin stain, revealed hyper-parakeratinized squamous epithelium with broad retepegs. The epithelium showed many dysplastic features like hyperchromatic nuclei, altered nuclear cytoplasmic ratio, loss of inter-cellular adherence and loss of stratification in one section. The underlying connective tissue showed marked inflammatory cells infiltrate with proliferative blood vessels and few areas with melanin pigments. Overall features suggested Oral Leukoplakia with moderate dysplasia (Figure 3). Suture removal done after 8 days. Healing was uneventful. Patient followed up after 30 days, 6 months and 1 year (Figure 2B). No recurrence reported.

Figure 2: (A) Excision of lesion (B) Follow up after a month.
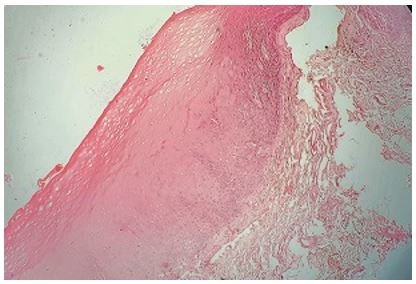
Figure 3: Histopathology picture showing moderately dysplastic lesion.
Oral cancer is the most commonly seen malignancy in Indian males and leukoplakia is the one of the commonest precancerous lesion of the oral cavity [4]. Leukoplakia is recently defined as “A predominantly white patch or plaque that cannot be characterized clinically or pathologically as any other disorder. Which carries an increased risk of cancer development either in the area of the leukoplakia or elsewhere in the oral cavity or the head-and-neck region” [5].
\ AetiologyTobacco in smoking and various other forms has been considered as the main incriminating factor. Other causative agents could be chronic irritation, lipstick, alcohol and ill-fitting dentures [4]. Role of Candida albicans as an aetiological factor and in malignant transformation is still uncertain. Viral agent’s role in the pathogenesis of oral leukoplakia particularly exophytic, verrucous leukoplakia has been noticed [1].
Age and genderOnset of leukoplakia commonly occur after 3rd decay of life, with a peak incidence above 5th decay. Different regions of India shows male predominance over female whereas Western countries show almost equal distribution [1].
Clinical patternLeukoplakia shows two types of clinical presentation Homogenous Pattern which is regular and uniform white surface with distinct borders. Homogenous clinical type shows a low risk to malignant transformation (5%). Non homogenous clinical Pattern includes leukoplakias with an red component (erythroleukoplakia), erosive, nodular, ulcerated and verrucous exophytic component [6].
HistopathologyMicroscopically it can show 1) hyperkeratosis (parakeratosis)with varying degree of dysplasia also carcinoma in situ and invasive carcinoma can be seen. 2) “Benign hyperkeratosis” with absence of dysplasia but show atrophy, or inflammation [7].
Histological grading of leukoplakia is based on degree of dysplasia which can be mild, moderate and severe depending on extent of involvement of epithelium [8]. Still there is lack of molecular markers or set of markers that would preciously confirmed the diagnosis of oral leukoplakia [9].
Malignant transformationAssociated risk factors for malignant transformation are clinical type, grade of dysplasia, age, size. Advancing age is found to be a main risk factor [2]. Erythroleukoplakia shows higher degree of malignant transformations than homogeneous leukoplakia. Although leukoplakia has male predominance females show significantly higher malignant transformation [2,3]. Size greater than 200 mm and location on the tongue and/or floor of the mouth will have increased of malignant transformation [7]. The reason for dysplasia grading was to determine and prevent malignant transformation. But, studies have been unable to effectively predict malignant transformation on the basis of degree of dysplasia [8].
TreatmentCessation of tobacco habits may result in regression of the lesion. It is rare to see Spontaneous disappearance of oral leukoplakia. Long standing cases and small lesions are conventionally treated by surgical removal. Nonsurgical treatment modalities include topical retinoids, beta-carotene, vitamin C supplements, 5-fluorouracil and bleomycin. Leukoplakia can be treated with newer treatment options such as cryosurgery, laser treatment, CO2 evaporation of excision and more recently a photodynamic therapy. Nonsurgical treatment sometimes may need to be used in long term so carry serious side effects. Irrespective to the type of treatment recurrences may occur so long term follow is recommended with cessation of tobacco habit [9].
The role of the dentist and oral medicine specialist is very important in the early diagnosis of premalignant lesion. Even a minute pathological change in oral epithelium should be screened and treated promptly even if it is asymptomatic so that simply removal of causative etiological factors results in decreased rate of malignant transformation. Case discussed above could have been gone unnoticed if did not examine properly or it could have been misdiagnosed as a traumatic hyperkeratosis. Even though it was very small in size and homogeneous the tiny lesion showed moderate dysplasia which is one of the major risk factor for malignant transformation. Early diagnosis and timely complete excision of such lesion gave very good prognosis. Generally complete excision of small lesion of leukoplakia is preferred and patients should be followed up to avoid chances of recurrence. Cessation of etiological factor especially tobacco should be strictly followed and alcohol consumption should be avoided.
Nil.
Citation: Lavanya Pasalkar., et al. “Unusual Clinical Presentation of Oral Leukoplakia: Case Report and Review of Literature”. Acta Scientific Dental Sciences 5.4 (2021): 196-199.
Copyright: © 2021 Lavanya Pasalkar., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.
