Manisha D Yadav1*, Bhakti Patil Soman2 and Deepa Das3
1Post Graduate Student, Oral Medicine and Radiology, G.D. Pol. Foundation Y.M.T.D.C, Navi Mumbai, Maharashtra, India
2Reader, Department of Oral Medicine and Radiology, G.D. Pol. Foundation Y.M.T.D.C, Navi Mumbai, Maharashtra, India
3Professor and HOD, Oral Medicine and Radiology, G.D. Pol. Foundation Y.M.T.D.C, Navi Mumbai, Maharashtra, India
*Corresponding Author: Manisha D Yadav, Post Graduate Student, Oral Medicine and Radiology, G.D. Pol. Foundation Y.M.T.D.C, Navi Mumbai, Maharashtra, India.
Received: March 10, 2021; Published: March 22, 2021
Dens Invaginatus, also known as dens in dente a rare developmental anomaly affecting human dentition. It arises as a result of invagination into the surface of tooth crown or root before calcification has occurred. Most commonly affected teeth are permanent maxillary lateral incisors and is usually seen on the palatal aspect. In the present case report it was, rare to be seen on the labial aspect of maxillary central incisor. This anomaly may increase the risk of pulp disease and can potentially complicate treatment due to its aberrant anatomy thus, posing a diagnostic challenge. Radiography plays a vital role in diagnosing such developmental anomaly. Compared to conventional radiograph Cone Beam Computed Tomography (CBCT) plays an invaluable role in the diagnosis of the extent dens invaginatus and in appropriate treatment planning. This case report highlights the role of CBCT in the diagnosis of various types of dens in dente.
Keywords: Dens Invaginatus; Dens in Dente; Labial; Maxillary Central Incisors; CBCT
CBCT: Cone Beam Computed Tomography; Kv: Kilovoltage; mA: Milliampere; irt: In Relation To
Dens Invaginatus is a rare developmental malformation resulting from invagination of the enamel organ into the dental papilla prior to calcification of the dental tissues [1]. Many terms have been used to describe this condition such as ‘dens in dente’, ‘dilated composite odontome’, ‘gestant anomaly’, deep foramen caecum and tooth inclusion [1,2]. Out of various nomenclature dens invaginatus would appear to be most appropriate as it reflects the infolding of the outer portion (enamel) into the inner portion (dentine) with the formation of a pocket or dead space [1].
Several theories have been put forward regarding etiology of dens invaginatus [3]:
It commonly occurs in maxillary permanent lateral incisors, followed by the maxillary central incisors, premolars, canines and less often in molars. Clinically, dens invaginatus appears in the crown at palatal side as deep pit which is prone to caries. Majority of cases have been reported in the literature were Dens invaginatus is on the palatal surface and only one case has been reported of Dens Invaginatus on the labial surface by Raut, Ambar W., et al. 2016 [5]. It is rarely seen in the mandibular teeth and deciduous teeth.3 In humans, dens invaginatus was first described by a dentist named Socrates in 1859.
The reported prevalence of adult teeth affected with dens invaginatus is between 0.3% and 10% with symptoms in 0.25% - 26.1% of individuals [3]. The most popularly known classification is Oehler’s classification, given in 1957. He described them as coronal invaginations and radicular invaginations and classified them as:
Radicular invaginations are rare and are thought to arise secondary to a proliferation of Hertwig’s root sheath with the formation of a strip of enamel that extends along the surface of the root [6].
Bhaskar describes two variations of dens invaginatus, coronal type and radicular type. The coronal type is caused by an invagination usually originate from an anomalous infolding of the enamel organ into the dental papilla. Radicular type results from an invagination of Hertwig’s epithelial root sheath which results in accentuation of normal longitudinal root groove. Mandibular first premolars and second molars are especially prone to develop the radicular variety. Compared to coronal type in radicular type, pulpal necrosis and apical lesions are more commonly associated [3].
The present case reports highlight the rare occurrence of dens invaginatus on the labial surface of the maxillary central incisor and role of CBCT in to diagnosing the extent and management of this developmental anomaly.
A 20-year-old male patient reported to the Department of Oral Medicine and Radiology at a private dental college and hospital with a chief complaint of abnormal tooth surface in the upper anterior region since childhood and wanted treatment for the same. On intraoral examination, a complex structure with deep pit was observed on the labial surface of left maxillary central incisor with tobacco stains (Figure 1a and 1b) and the tooth responded negatively to vertical percussion. The patient had a non- contributory family and medical history. So, based on clinical findings a provisional diagnosis of Dens Invaginatus was given. Radiographic investigation was carried out to diagnose the extent of invagination. On examining Intraoral periapical radiograph, it showed the presence of pear shape radiopacity which tapered coronally suggestive of dens invaginatus in relation to left maxillary central incisor (Figure 2). For detail radiographic examination Cone Beam Computed Tomography Scan of maxillary anterior region was also performed with the Kodak 9000C 3D Volumetric Tomography (Carestream Health INC. Rochester, NY USA), with exposure parameters 74Kv, 12mA, 10 seconds with Field of view 5 x 5. Image reconstruction was made by the Carestream 3D Imaging Software (Atlanta, GA, USA) which revealed a hyperdense mass incisally on the labial surface of 21 with linear hypodensity about 1.5 mm confined to the crown structure which was not in continuity with the main root canal. Hyperdensity noted was similar to enamel of tooth irt 21. Large pulp chamber with single root canal was observed on CBCT scan (Figure 3a-3f). Radiographic diagnosis of Oehlers Type I dens invaginatus on labial surface irt 21 was made.

Figure 1a and 1b: Dens Invaginatus on labial surface of 21 with no anomaly on palatal surface.

Figure 2: Intraoral periapical radiograph irt 11 & 21.
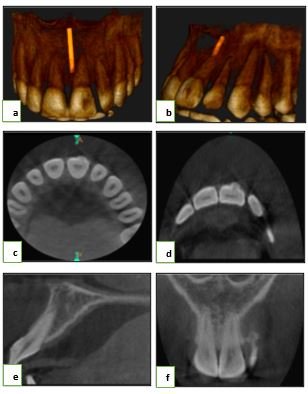
Figure 3a-3f: CBCT scan showing 3D reconstruction image, axial, sagittal and coronal plane of Oehlers Type I Dens Invaginatus on labial surface irt 21.
Dens invaginatus is clinically important as the altered anatomy makes dental caries to easily reach the pulp chamber. Clinically it is seen as a deep palatal pit and it is difficult to diagnose. Cases that have been reported in the literature indicate that the condition is fairly common and that an extremely wide range in degree of variation can exist. Most of the time it is usually detected with the help of intraoral periapical radiographs. 2-dimensional radiography does not provide much detail regarding the extent of invagination, they just provide 2D view of the complex anatomy. So, Cone Beam Computed Tomography (CBCT) plays a valuable role in imaging the extent of invagination and its relationship with the main root canal of the affected tooth and thereby play a vital role in treatment planning. Dens Invagination usually occurs bilaterally involving central and lateral incisors. But in the present case, it was seen on the labial surface of left maxillary central incisor. To best of my knowledge there is only one case reported in the literature of labial type dens invaginatus of maxillary lateral incisor [5]. Microorganisms usually pass from oral cavity through dens invaginatus into the pulp leading to abscess formation, cyst development, tooth displacement and internal resorption if left untreated. Early diagnosis of this anomaly is crucial as it aids in better prognostic treatment modality. Pulp vitality test should be performed in suspected cases. If the results suggest vital and unaffected pulpal tissue, then the teeth should be restored. Management of dens invaginatus includes prophylactic restoration to conventional endodontic treatment or extraction, depending on the type of invagination, function, esthetics and morphology of the root canal. Extraction is indicated as a last choice of treatment in cases of failure of root canal treatment and in supernumerary teeth associated with dens invaginatus [3,7-16].
Dens invaginatus is generally underdiagnosed and in most of cases is detected by chance on radiograph. Only one cases of labial type of Dens Invaginatus have been reported in the literature so far [5]. Present case is the second case report of labial type Dens Invaginatus. Also, Cone Beam Computed Tomography have been successfully used in early diagnosis and management of this developmental anomaly.
There is no conflict of interest.
Citation: Manisha D Yadav., et al. “Labial Type Dens in Dente: A Rare Case Report”. Acta Scientific Dental Sciences 5.4 (2021): 192-195.
Copyright: © 2021 Manisha D Yadav., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

















 Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Open Access by
Acta Scientific is licensed under a Creative Commons Attribution 4.0 International License
Based on a work at https://actascientific.com
ff
ff
© 2024 Acta Scientific, All rights reserved.
